Prathapadas Unnikrishnan, Hrishi Ajay Prasad, Appavoo Arulvelan, Vimala Smita, Sethuraman Manikandan
Division of Neuroanaesthesia, Department of Anaesthesiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, India.
Department of Neuro Anaesthesiology, Institute of Neuro Sciences, SIMS Hospital, Chennai, India.
J Neurosci Rural Pract. 2020 Apr;11(2):267-273. doi: 10.1055/s-0040-1703968. Epub 2020 Mar 17.
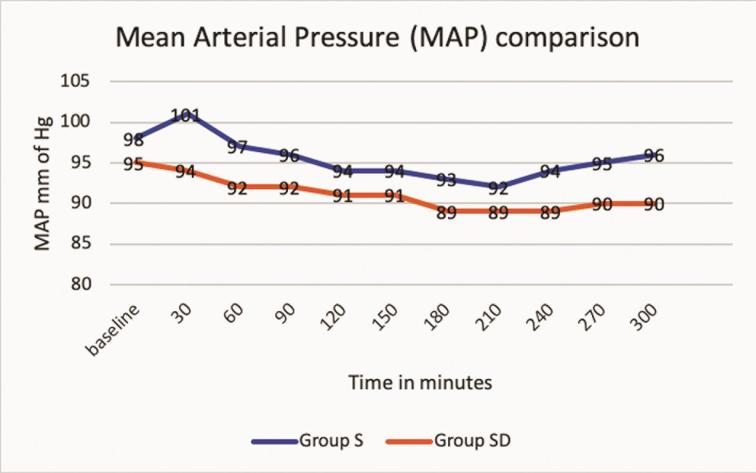
Dexmedetomidine could be a suitable adjuvant in neuroanesthesia due to its analgesic and anesthetic-sparing properties with the added advantage of facilitating intraoperative neuromonitoring. However, its recovery profile is still debated upon, as in neuroanesthesia, a prompt recovery is essential for postoperative neurologic assessment. We designed this study to evaluate the effect of dexmedetomidine on the anesthetic and recovery profile of patients presenting for supratentorial neurosurgeries. Forty adult patients undergoing supratentorial surgeries were recruited in this prospective, randomized, double-blinded study and were divided into two groups: group S and group SD. Both groups received sevoflurane and fentanyl for maintenance, whereas group SD alone received a low dose of dexmedetomidine infusion. Recovery parameters, opioid consumption, Richmond Agitation-Sedation Scale (RASS) and visual analogue scale (VAS) scores, incidence of nausea and vomiting, and intraoperative hemodynamics were analyzed. There were no statistically significant differences between the groups S and SD in case of recovery parameters-time taken (in minutes, presented as median with interquartile range [IQR]) for (1) eye-opening to command: 9.5 (8-18) versus 22.5 (5-47.5) ( = 0.414); 2) following verbal command: 10.5 (8.25-29.5) versus 25 (10-28.75) ( = 0.512); (3) extubation: 11 (9.25-22) versus 25 (10-30) ( = 0.277); and (4) getting oriented to place, time, and date: 23 (20-52.75) versus 27.5 (25-36.5) ( = 0.121). Fentanyl consumption was significantly less in group SD (451 ± 39.3) versus group S (524.3 ± 144.1) ( = 0.034). The median RASS score with IQR and the median VAS scores with IQR were comparable between the groups at all time points. Of the 20 patients in group S, 5 had complaints of nausea and vomiting compared with none in the group SD, although it was not statistically significant. The hemodynamic parameters did not show a significant difference between the groups except for a surge in mean arterial pressure at 30 minutes in group S. Low-dose dexmedetomidine as an adjuvant to sevoflurane- and fentanyl-based anesthesia could provide stable hemodynamics and lesser anesthetics and opioid consumption, without adversely affecting the recovery profile in patients undergoing supratentorial neurosurgical procedures.
右美托咪定因其具有镇痛和节省麻醉药物的特性,且有助于术中神经监测,可能是神经麻醉中一种合适的辅助药物。然而,其恢复情况仍存在争议,因为在神经麻醉中,快速恢复对于术后神经功能评估至关重要。我们设计了这项研究,以评估右美托咪定对幕上神经外科手术患者麻醉和恢复情况的影响。
在这项前瞻性、随机、双盲研究中,招募了40例接受幕上手术的成年患者,并将其分为两组:S组和SD组。两组均使用七氟烷和芬太尼维持麻醉,而SD组单独接受低剂量右美托咪定输注。分析了恢复参数、阿片类药物用量、Richmond躁动-镇静量表(RASS)和视觉模拟量表(VAS)评分、恶心和呕吐的发生率以及术中血流动力学。
S组和SD组在恢复参数方面无统计学显著差异,即(1)对指令睁眼所需时间(分钟,以中位数和四分位间距[IQR]表示):9.5(8 - 18)对22.5(5 - 47.5)(P = 0.414);(2)对言语指令有反应所需时间:10.5(8.25 - 29.5)对25(10 - 28.75)(P = 0.512);(3)拔管时间:11(9.25 - 22)对25(10 - 30)(P = 0.277);以及(4)对地点、时间和日期定向所需时间:23(20 - 52.75)对27.5(25 - 36.5)(P = 0.121)。SD组的芬太尼用量(451 ± 39.3)明显低于S组(524.3 ± 144.1)(P = 0.034)。两组在所有时间点的RASS评分中位数及IQR和VAS评分中位数及IQR均具有可比性。S组的20例患者中有5例出现恶心和呕吐,而SD组无此情况,尽管差异无统计学意义。除S组在30分钟时平均动脉压有波动外,两组的血流动力学参数无显著差异。
低剂量右美托咪定作为七氟烷和芬太尼麻醉的辅助药物,可提供稳定的血流动力学,减少麻醉药物和阿片类药物的用量,且不会对幕上神经外科手术患者的恢复情况产生不利影响。