Larson Christopher M, Williams Brady T, Bessa Felipe, McGaver Rebecca Stone, Suppauksorn Sunikom, Faucett Scott, Chahla Jorge
Twin Cities Orthopedics, Edina, Minnesota, U.S.A.
Rush University Medical Center, Chicago, Illinois, U.S.A.
Arthrosc Tech. 2020 Mar 11;9(4):e453-e458. doi: 10.1016/j.eats.2019.11.019. eCollection 2020 Apr.
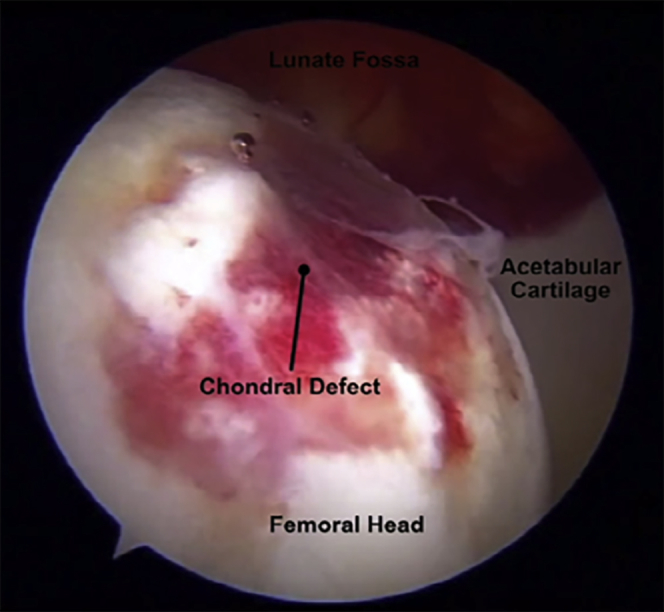
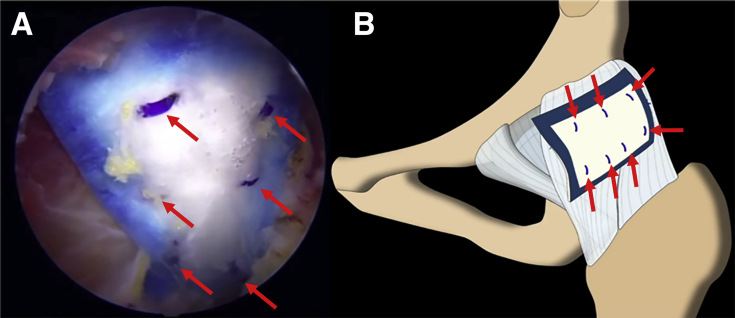
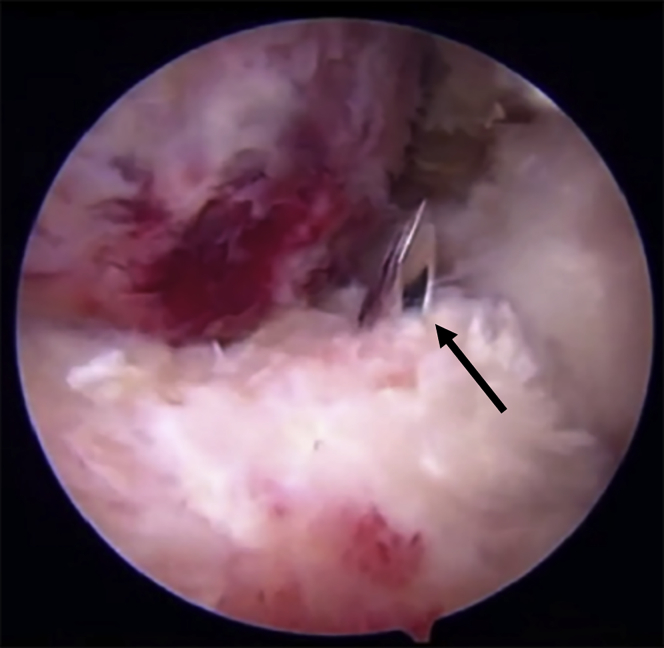
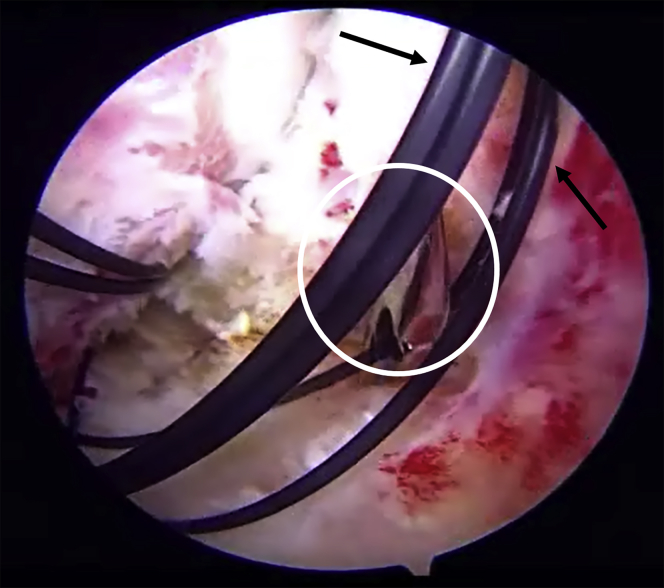
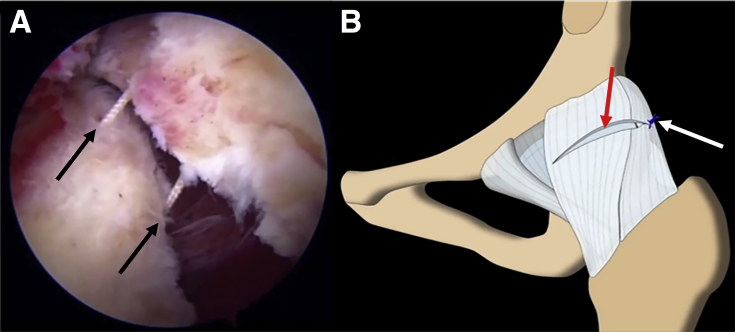
In the past decade, the number of hip arthroscopy procedures has exponentially increased, primarily for the treatment of femoroacetabular impingement syndrome and labral lesions. As the techniques have evolved, so has the acknowledgment of the potential complications, including iatrogenic instability that may result from soft-tissue laxity, subtle dysplastic morphologies, or residual defects from capsulotomies in which the capsular closure is insufficient. In most cases, direct capsular repair or plication can be performed at the conclusion of the procedure; however, larger defects, poor-quality tissue, or cases of gross ligamentous laxity may require reconstruction or augmentation. In such instances, several options exist. The purpose of this technical note is to describe a capsular repair augmentation with a bioinductive implant during revision hip arthroscopy.
在过去十年中,髋关节镜手术的数量呈指数级增长,主要用于治疗股骨髋臼撞击综合征和盂唇损伤。随着技术的发展,人们对潜在并发症的认识也在增加,包括可能由软组织松弛、轻微发育不良形态或关节囊切开术后残留缺陷(其中关节囊闭合不充分)导致的医源性不稳定。在大多数情况下,可在手术结束时进行直接的关节囊修复或折叠;然而,较大的缺损、质量较差的组织或严重韧带松弛的病例可能需要重建或增强。在这种情况下,有几种选择。本技术说明的目的是描述在翻修髋关节镜检查期间使用生物诱导植入物进行关节囊修复增强的方法。