Johns Hopkins University School of Nursing, 525 North Wolfe St., Rm 426, Baltimore, MD, 21205, USA.
Johns Hopkins Bloomberg School of Public Health Department of Health Policy and Management, Baltimore, USA.
BMC Geriatr. 2020 May 6;20(1):156. doi: 10.1186/s12877-020-01553-4.
Less educational training is consistently associated with incident dementia among older adults, but associations between income and financial strain with incident dementia have not been well tested in national samples. This is an important gap because, like education, financial resources are potentially modifiable by policy change and strengthening the social safety net. This study tested whether financial resources (income and financial strain) predict six-year incident dementia independent of education and occupation.
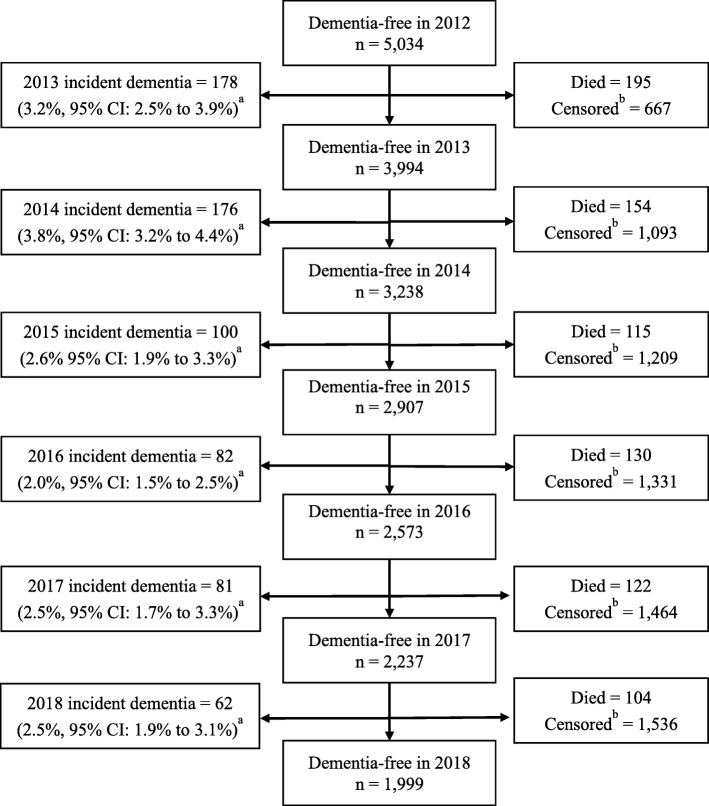
The National Health and Aging Trends Study is a prospective cohort study that recruited a nationally representative sample of U.S. Medicare beneficiaries aged ≥65 years. Incident dementia (2013 to 2018) was classified based on diagnosis, cognitive test scores or proxy-reported changes among participants dementia-free in 2012 (n = 3785). Baseline socioeconomic measures included income to poverty ratio (analyzed separately for those < 500% vs. ≥500% poverty threshold), financial strain, education and history of professional occupation. Discrete time survival analysis applied survey weights to account for study design and nonresponse. Coefficients were standardized to compare the strength of associations across the four socioeconomic measures.
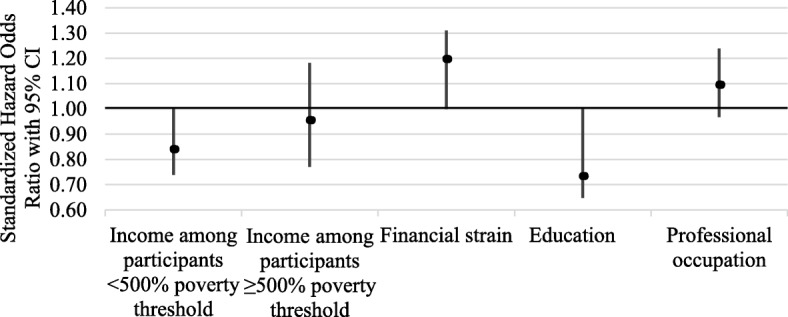
Adjusting for socioeconomic measures, demographic characteristics, home ownership, retirement, chronic conditions, smoking, BMI and depressive symptoms, higher income (hazard OR = 0.84, 95% CI: 0.74, 0.95 among those < 500% poverty) and higher education (hOR = 0.73, 95% CI: 0.65, 0.83) were associated with lower odds, and financial strain with higher odds (hOR = 1.20, 95% CI: 1.09, 1.31), of incident dementia.
Low income and greater financial strain predict incident dementia among older adults and associations are comparable to those of low education among U.S. older adults. Interventions to mitigate financial strain through improving access to economic opportunity and strengthening safety net programs and improving access to them in low income groups may complement other ongoing efforts to prevent dementia.
在老年人中,教育程度较低与痴呆症的发生呈一致相关,但收入和经济压力与痴呆症发生之间的关联在全国样本中尚未得到充分验证。这是一个重要的差距,因为与教育一样,经济资源可以通过政策改变和加强社会安全网来改变。本研究测试了财务资源(收入和经济压力)是否可以独立于教育和职业预测六年内的痴呆症发病情况。
国家健康老龄化趋势研究是一项前瞻性队列研究,招募了美国医疗保险受益人的全国代表性样本,年龄≥65 岁。根据 2012 年无痴呆症的参与者(n=3785)的诊断、认知测试评分或代理报告的变化,将痴呆症的发生(2013 年至 2018 年)分类。基线社会经济措施包括收入与贫困比例(<500%和≥500%贫困线的人分别分析)、经济压力、教育和职业历史。离散时间生存分析应用调查权重来考虑研究设计和无应答情况。对系数进行标准化,以比较四种社会经济措施之间关联的强度。
在调整社会经济措施、人口统计学特征、住房所有权、退休、慢性疾病、吸烟、BMI 和抑郁症状后,较高的收入(<500%贫困线的人,风险比 OR=0.84,95%可信区间:0.74,0.95)和较高的教育(hOR=0.73,95%可信区间:0.65,0.83)与较低的发病风险相关,而经济压力与较高的发病风险相关(hOR=1.20,95%可信区间:1.09,1.31)。
低收入和更大的经济压力预测了老年人的痴呆症发病,其相关性与美国老年人的低教育水平相当。通过改善获取经济机会和加强安全网计划的机会,缓解经济压力的干预措施,并改善低收入群体获取这些计划的机会,可能会补充其他预防痴呆症的现有努力。