Abiko Takehiro, Ebihara Yuma, Takeuchi Motoya, Sakamoto Hiroki, Homma Hisato, Hirano Satoshi
Gastroenterological Surgery, Sapporo Kyoritsu Gorinbashi Hospital, 1-chome, Kawazoe 1-jo, Minami-ku, Sapporo, Hokkaido, 0050802, Japan.
Department of Gastroenterological Surgery II, Hokkaido University Faculty of Medicine, North 15 West 7, Kita-ku, Sapporo, Hokkaido, 0608638, Japan.
Surg Case Rep. 2020 May 5;6(1):91. doi: 10.1186/s40792-020-00837-6.
Biliary bleeding is a condition reported by Sandblom as hemobilia. The most common cause of hemobilia is iatrogenicity. But it has also been reported as a rare complication after laparoscopic cholecystectomy (LC).
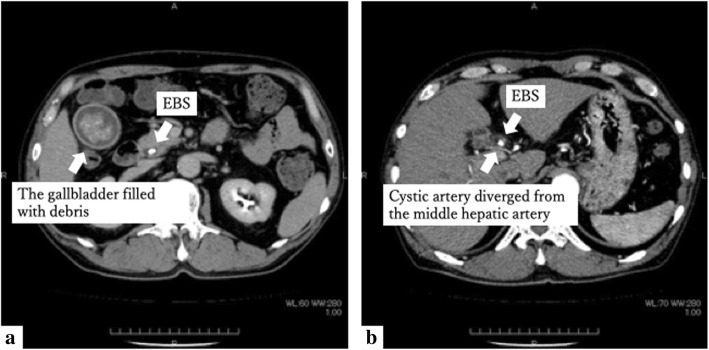
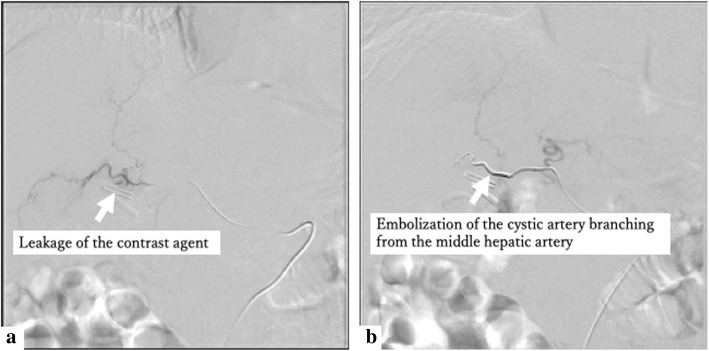
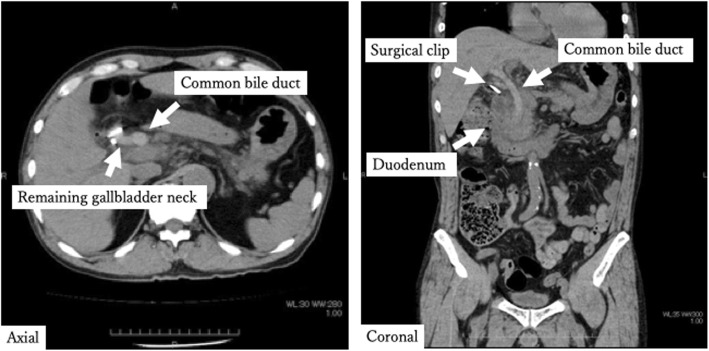
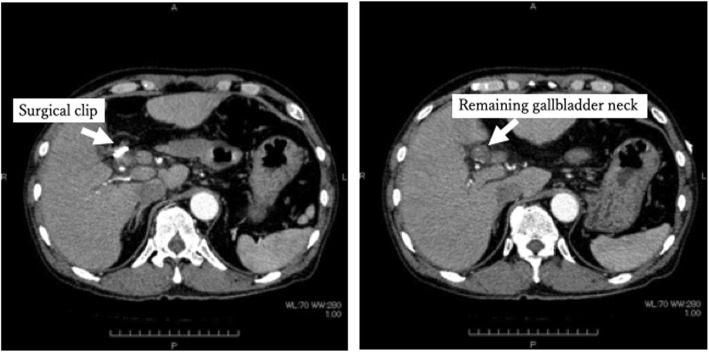
A man in his 60s underwent a LC. He was taking a direct Xa inhibitor for paroxysmal atrial fibrillation (pAf) and had a history of thrombectomy. There was variation in the bifurcation of the hepatic artery and cystic artery. The right hepatic artery branches from the common hepatic artery by itself, and the cystic artery is double. He complained of right upper quadrant pain, nausea, and vomiting on the third postoperative day (3POD). Non-contrast computed tomography (CT) showed that a high absorption area was found to fill the common bile duct. Contrast CT showed no pseudoaneurysm formation. Ultimately, he was diagnosed with postoperative hemobilia. Angiographic examination selective for the cystic artery branching from the middle hepatic artery revealed leakage of the contrast agent and a micro-pseudoaneurysm.
We encountered a case of hemobilia after LC. In this case, it was presumed that in addition to the chronic inflammatory changes of the gallbladder wall, extraordinary bifurcation of the hepatic artery and the cystic arteries and easy bleeding due to resumption of a direct Xa inhibitor synergistically caused a micro-pseudoaneurysm and postoperative hemobilia. It was difficult to identify the cause of hemobilia by contrast CT alone. Angiographic examination was useful for identifying and treating the causative artery and needs to perform aggressively.
胆道出血是桑德布洛姆报道的一种被称为血胆症的病症。血胆症最常见的病因是医源性的。但它也被报道为腹腔镜胆囊切除术(LC)后一种罕见的并发症。
一名60多岁的男性接受了LC手术。他正在服用直接Xa因子抑制剂治疗阵发性心房颤动(pAf),并有血栓切除术史。肝动脉和胆囊动脉的分叉存在变异。右肝动脉独自从肝总动脉分支,胆囊动脉为双支。术后第3天(3POD),他出现右上腹疼痛、恶心和呕吐。非增强计算机断层扫描(CT)显示胆总管内有一个高密度影填充区。增强CT显示无假性动脉瘤形成。最终,他被诊断为术后血胆症。对发自肝中动脉的胆囊动脉进行选择性血管造影检查发现造影剂渗漏和一个微假性动脉瘤。
我们遇到了一例LC术后血胆症病例。在本病例中,推测除胆囊壁的慢性炎症改变外,肝动脉和胆囊动脉的异常分叉以及直接Xa因子抑制剂恢复使用导致的易出血状态协同作用,导致了微假性动脉瘤和术后血胆症。仅通过增强CT很难确定血胆症的病因。血管造影检查对于识别和治疗致病动脉很有用,需要积极进行。