Department of Gastrointestinal Surgery, Shinko Hospital, 1-4-47, Wakinohama-cho, Chuo-ku, Kobe, Hyogo, 6510072, Japan.
Department of Gastroenterology, Shinko Hospital, 1-4-47, Wakinohama-cho, Chuo-ku, Kobe, Hyogo, 6510072, Japan.
BMC Surg. 2021 Aug 5;21(1):318. doi: 10.1186/s12893-021-01314-z.
Hemobilia refers to bleeding into the biliary tract. Hepatic artery pseudoaneurysm (HAP) rupture is an uncommon cause of hemobilia, and cases of HAP associated with Mirizzi syndrome are extremely rare. Although transarterial embolization is recommended as the first-line treatment for hemobilia, surgery is sometimes required.
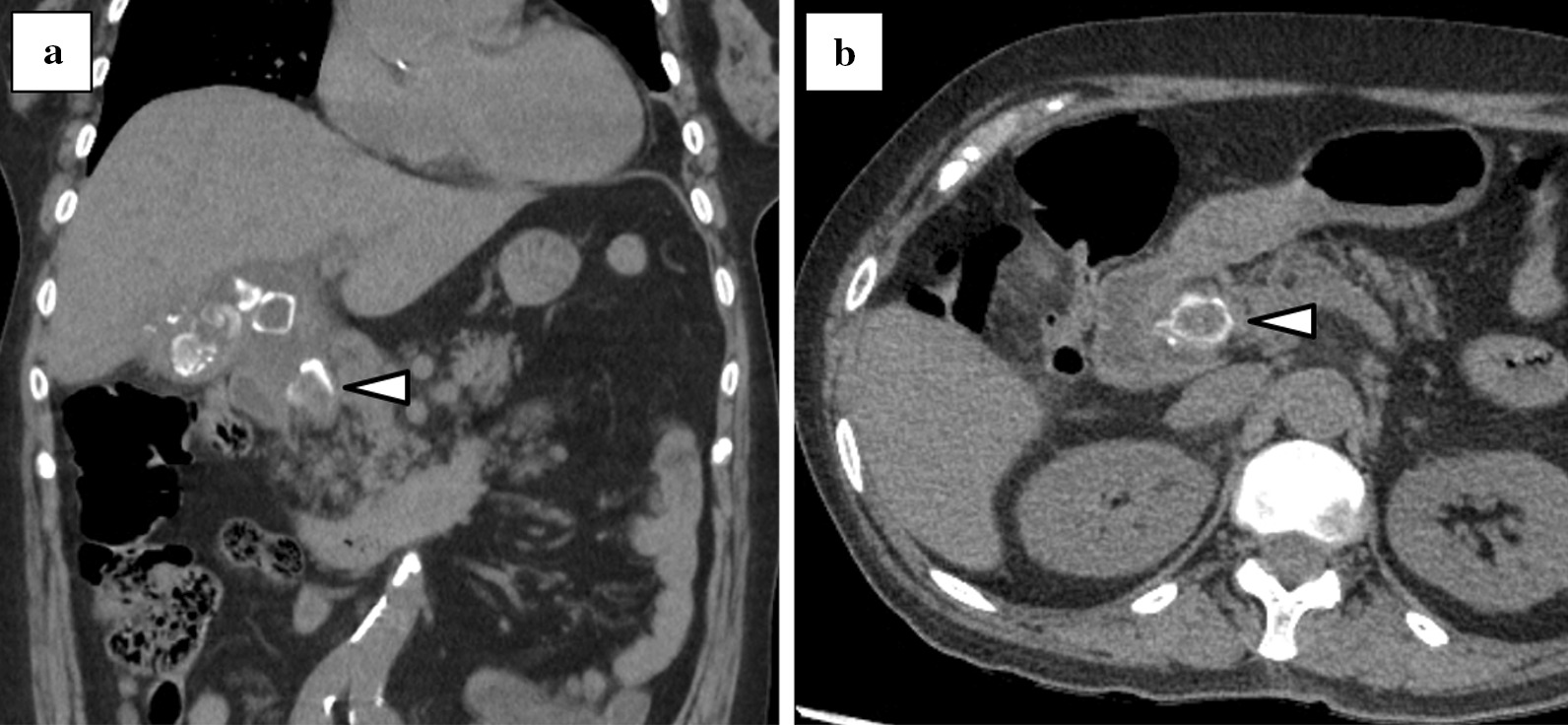
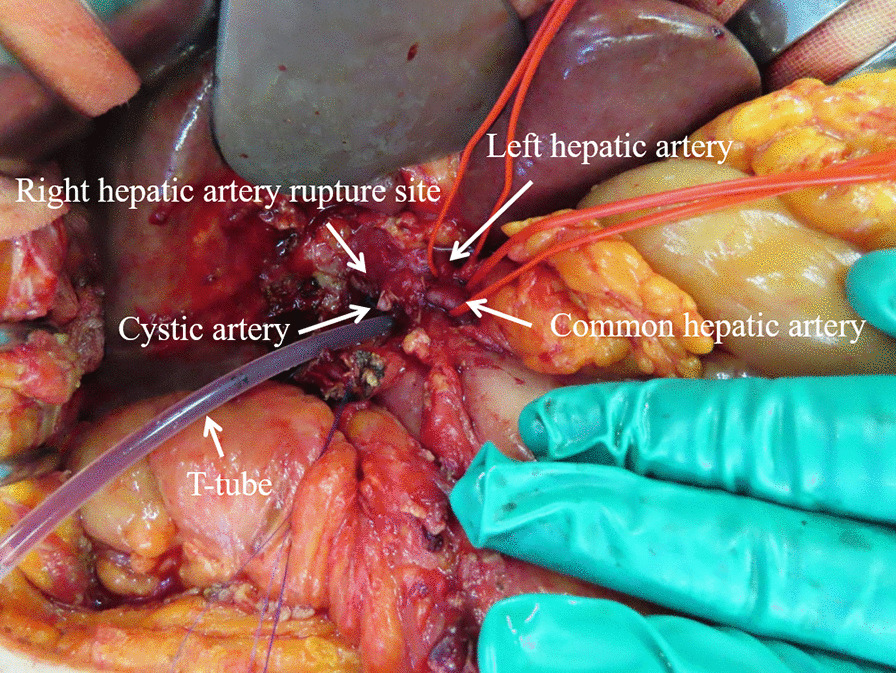
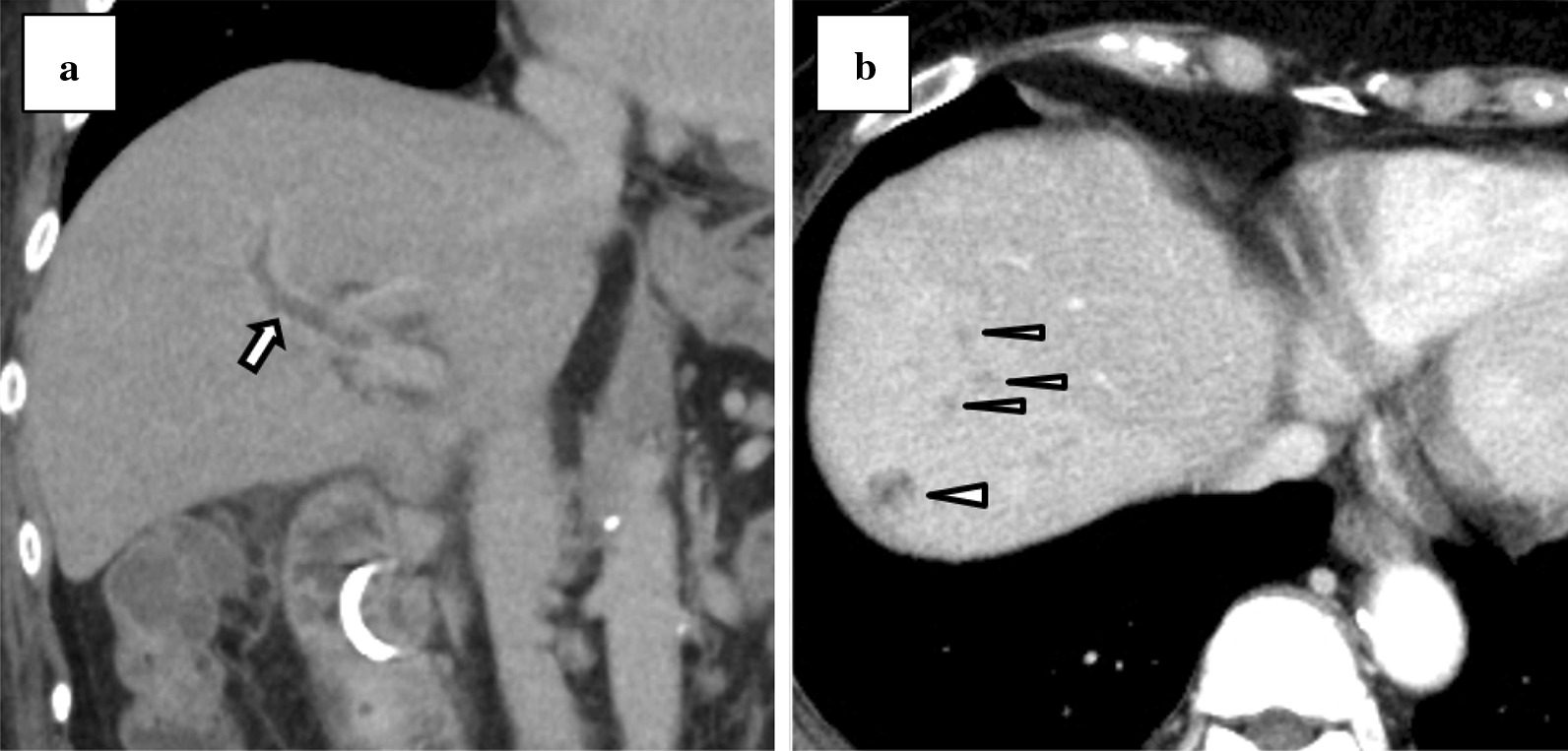
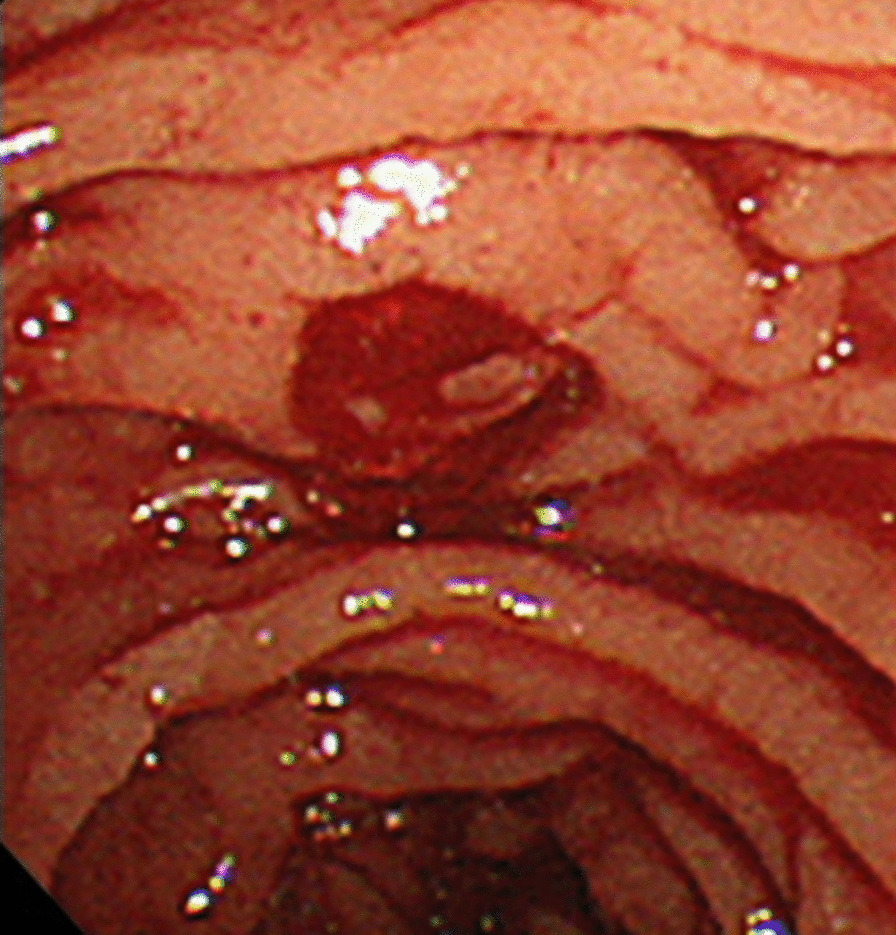
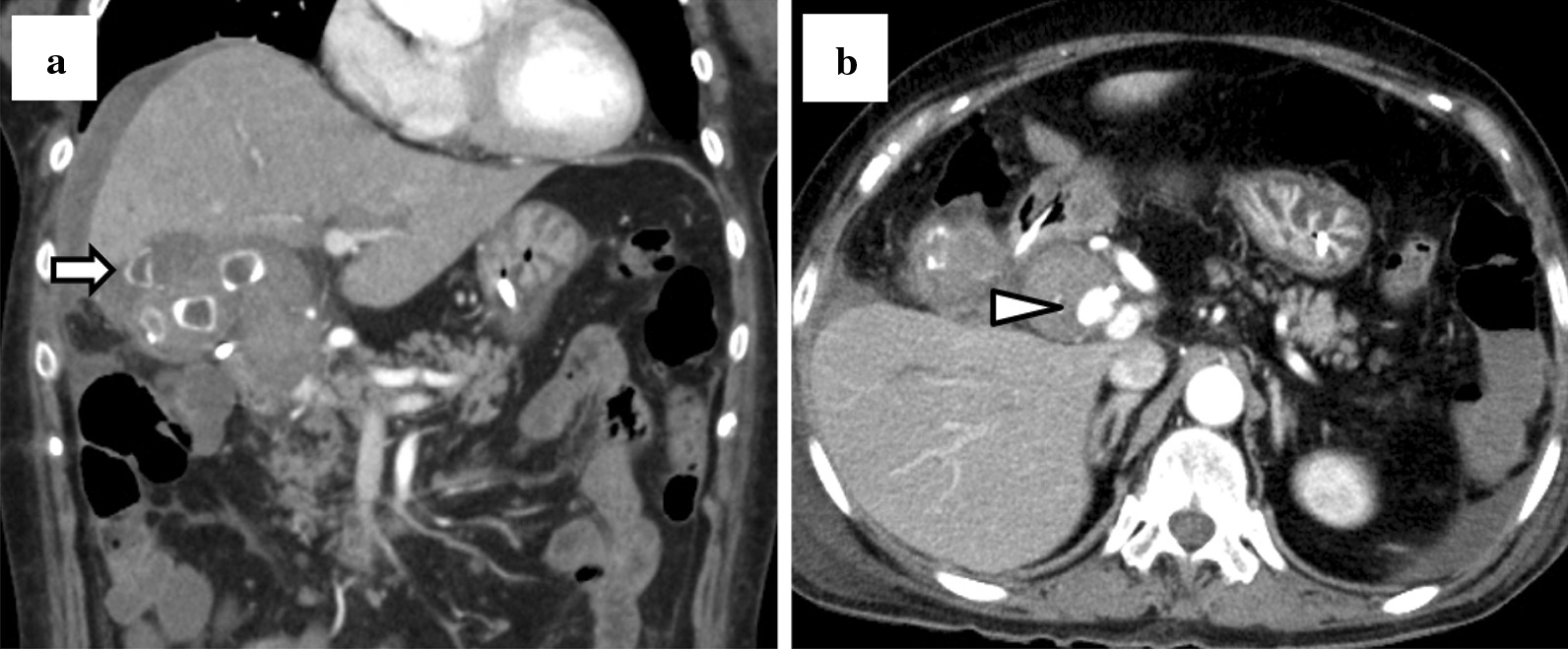
A 76-year-old woman was referred to our hospital with epigastric pain. She was febrile and had conjunctival icterus and epigastric tenderness. Laboratory tests revealed abnormal white blood cell count and liver function. An abdominal computed tomography (CT) revealed multiple calculi in the gallbladder, an incarcerated calculus in the cystic duct, and a slightly dilated common hepatic duct. Based on examination findings, she was diagnosed with Mirizzi syndrome type I, complicated by cholangitis. Intravenous antibiotics were administered, and we performed endoscopic retrograde cholangiopancreatography (ERCP) to place a drainage tube. The fever persisted; therefore, contrast-enhanced CT (CECT) was performed. This revealed portal vein thrombosis and hepatic abscesses; therefore, heparin infusion was administered. The following day, she complained of melena, and laboratory tests showed that she was anemic. ERCP was performed to change the drainage tube in the bile duct; however, bleeding from the papilla of Vater was observed. CECT demonstrated a right HAP with high-density fluid in the gallbladder and gallbladder perforation. Finally, she was diagnosed with hemobilia caused by HAP rupture, and emergency surgery was performed to secure hemostasis and control the infection. During laparotomy, we found that a right HAP had ruptured into the gallbladder. The gallbladder made a cholecystobiliary fistula, which indicated Mirizzi syndrome type II. Although we tried to repair the right hepatic artery, we later ligated it due to arterial wall vulnerability. Then, we performed subtotal cholecystectomy and inserted a T-tube into the common bile duct. There were no postoperative complications except for minor leakage from the T-tube insertion site. The patient was discharged after a total hospital stay of 7 weeks.
We experienced an extremely rare case of emergency definitive surgery for hemobilia due to HAP rupture complicated by Mirizzi syndrome type II. Surgery might be indicated when controlling underlying infections was required.
血胆汁是指血液进入胆道。肝动脉假性动脉瘤(HAP)破裂是血胆汁的一个不常见原因,而与 Mirizzi 综合征相关的 HAP 极为罕见。尽管经动脉栓塞被推荐为血胆汁的一线治疗方法,但有时仍需要手术。
一名 76 岁女性因上腹痛就诊。她发热,结膜发黄,上腹部压痛。实验室检查显示白细胞计数和肝功能异常。腹部 CT 显示胆囊内多发结石,胆囊管嵌顿结石,胆总管轻度扩张。根据检查结果,诊断为 Mirizzi 综合征 I 型,合并胆管炎。给予静脉抗生素治疗,并进行内镜逆行胰胆管造影(ERCP)以放置引流管。发热持续,因此进行了增强 CT(CECT)检查。结果显示门静脉血栓形成和肝脓肿,因此给予肝素输注。第二天,患者诉黑便,实验室检查显示贫血。进行 ERCP 以更换胆管引流管,但观察到 Vater 乳头出血。CECT 显示 HAP 右侧,胆囊内高密度液体和胆囊穿孔。最终诊断为 HAP 破裂引起的血胆汁,行急诊手术止血和控制感染。剖腹探查时,发现 HAP 右侧破裂入胆囊。胆囊与胆管形成胆瘘,提示 Mirizzi 综合征 II 型。虽然我们试图修复右肝动脉,但由于动脉壁脆弱,后来还是结扎了。然后,我们进行了胆囊次全切除术,并在胆总管内插入 T 管。除 T 管插入部位轻微渗漏外,患者无术后并发症。患者共住院 7 周后出院。
我们遇到了一例极为罕见的因 HAP 破裂引起的血胆汁急症确定性手术的病例,合并 Mirizzi 综合征 II 型。当需要控制潜在感染时,手术可能是必要的。