Advanced Neuroscience Network/Tenet South Florida, Delray Beach, Florida, USA
Cerebrovascular Program, Vanderbilt University Medical Center, Nashville, Tennessee, USA.
J Neurointerv Surg. 2020 Nov;12(11):1058-1063. doi: 10.1136/neurintsurg-2019-015593. Epub 2020 May 8.
Routing patients directly to endovascular capable centers (ECCs) would decrease time to mechanical thrombectomy (MT), but may delay intravenous thrombolysis (IVT).
To study the clinical outcomes of patients with a stroke transferred directly to ECCs compared with those transferred to ECCs from non-endovascular capable centers (nECCs).
Data from the STRATIS registry were analyzed to evaluate process and clinical outcomes under five routing policies: (1) transport to nearest nECC; (2) transport to STRATIS ECC over any distance or (3) within 20 miles; (4) transport to ideal ECC (iECC), over any distance or (5) within 20 miles.
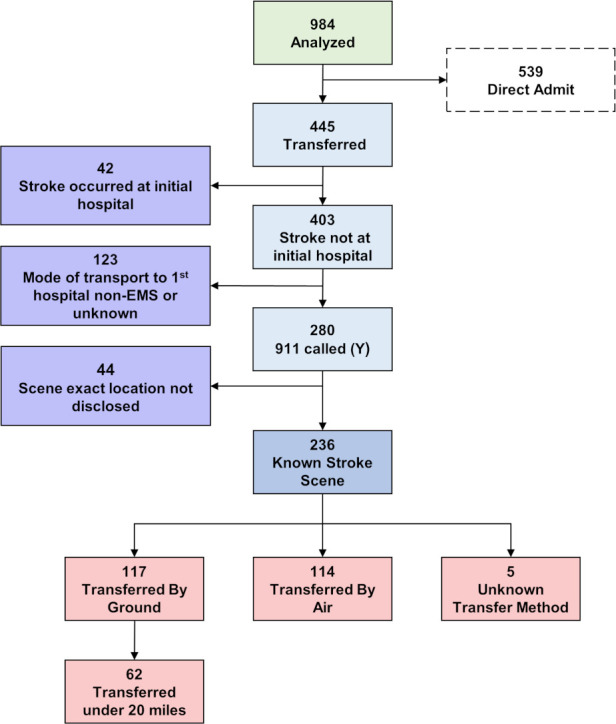
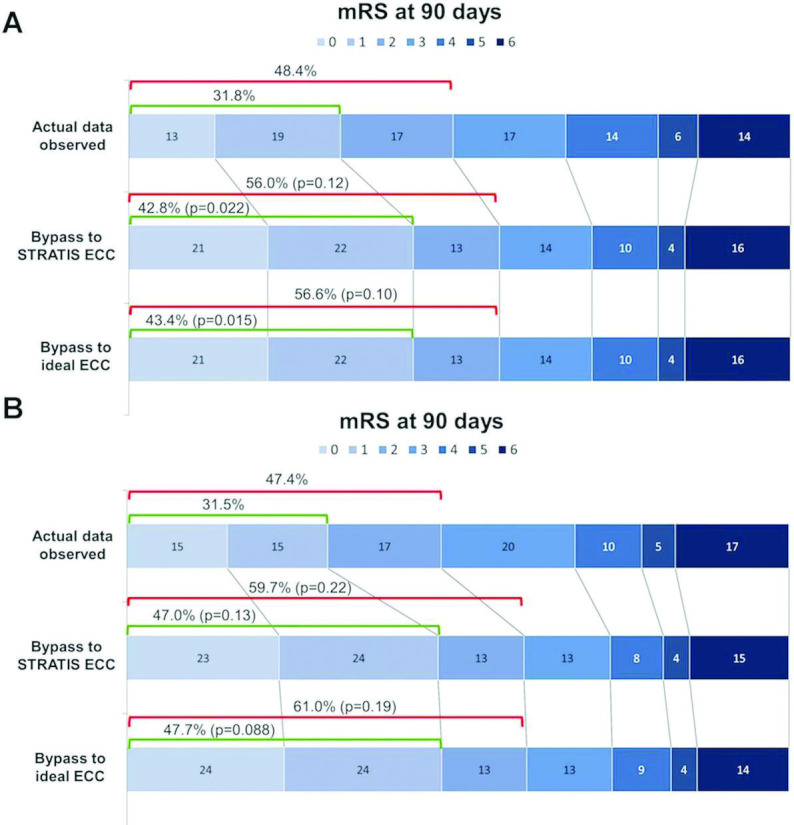
Among 236 patients, 117 (49.6%) were transferred by ground, of whom 62 (53%) were transferred within 20 miles. Median MT start time was accelerated in all direct transport models. IVT start was prolonged with direct transport across all distances, but accelerated with direct transport to iECC ≤20 miles. With bypass limited to ≤20 miles, the median modeled EMS arrival to IVT interval decreased for both iECCs and ECCs (by 12 min and 6 min, respectively), and median EMS arrival to puncture time decreased by up to 94 min. In this cohort, no patient would have become ineligible for IVT. Bypass to iECC modeling under 20 miles showed a significant reduction in the level of disability at 3 months, with freedom from disability (modified Rankin Scale score 0-1) at 3 months increased by 12%.
Direct routing of patients with a large vessel occlusion to ECCs, especially when within 20 miles, may lead to better clinical outcomes by accelerating the start of MT without any delay of IVT.
http://www.clinicaltrials.gov. Unique identifier: NCT02239640.
将患者直接转至血管内治疗中心(ECC)可缩短机械取栓(MT)时间,但可能会延迟静脉溶栓(IVT)。
研究直接转至 ECC 的患者与转至非血管内治疗中心(nECC)的患者相比的临床结局。
分析 STRATIS 注册研究的数据,以评估在五种转运行动方案下的流程和临床结局:(1)转送至最近的 nECC;(2)不论距离远近,均转送至 STRATIS ECC;(3)转送至 STRATIS ECC 距离不超过 20 英里;(4)不论距离远近,均转送至理想 ECC(iECC);(5)转送至 iECC 距离不超过 20 英里。
在 236 名患者中,有 117 名(49.6%)通过地面转运,其中 62 名(53%)在 20 英里内转运。所有直接转运模型均加速了 MT 开始时间。直接跨距转运均延长了 IVT 开始时间,但直接转运至 iECC 距离不超过 20 英里时可加速 IVT 开始。在限制转院距离不超过 20 英里的情况下,iECC 和 ECC 的中位模拟 EMS 到 IVT 间隔均缩短(分别为 12 分钟和 6 分钟),EMS 到达穿刺时间中位数缩短了最多 94 分钟。在本队列中,没有患者将失去 IVT 的资格。在 20 英里内对 iECC 进行旁路建模显示,3 个月时残疾程度显著降低,3 个月时无残疾(改良 Rankin 量表评分 0-1)的比例增加了 12%。
对于大血管闭塞患者,将其直接转至 ECC,尤其是在 20 英里内,可能会通过加速 MT 的启动而不会延迟 IVT,从而获得更好的临床结局。