Kahn Justine M, Brazauskas Ruta, Tecca Heather R, Bo-Subait Stephanie, Buchbinder David, Battiwala Minoo, Flowers Mary E D, Savani Bipin N, Phelan Rachel, Broglie Larisa, Abraham Allistair A, Keating Amy K, Daly Andrew, Wirk Baldeep, George Biju, Alter Blanche P, Ustun Celalettin, Freytes Cesar O, Beitinjaneh Amer M, Duncan Christine, Copelan Edward, Hildebrandt Gerhard C, Murthy Hemant S, Lazarus Hillard M, Auletta Jeffery J, Myers Kasiani C, Williams Kirsten M, Page Kristin M, Vrooman Lynda M, Norkin Maxim, Byrne Michael, Diaz Miguel Angel, Kamani Naynesh, Bhatt Neel S, Rezvani Andrew, Farhadfar Nosha, Mehta Parinda A, Hematti Peiman, Shaw Peter J, Kamble Rammurti T, Schears Raquel, Olsson Richard F, Hayashi Robert J, Gale Robert Peter, Mayo Samantha J, Chhabra Saurabh, Rotz Seth J, Badawy Sherif M, Ganguly Siddhartha, Pavletic Steven, Nishihori Taiga, Prestidge Tim, Agrawal Vaibhav, Hogan William J, Inamoto Yoshihiro, Shaw Bronwen E, Satwani Prakash
Division of Pediatric Hematology, Oncology and Stem Cell Transplantation, Department of Pediatrics, Columbia University, New York, NY.
Center for International Blood and Marrow Transplant Research, Department of Medicine, and.
Blood Adv. 2020 May 12;4(9):2084-2094. doi: 10.1182/bloodadvances.2019000839.
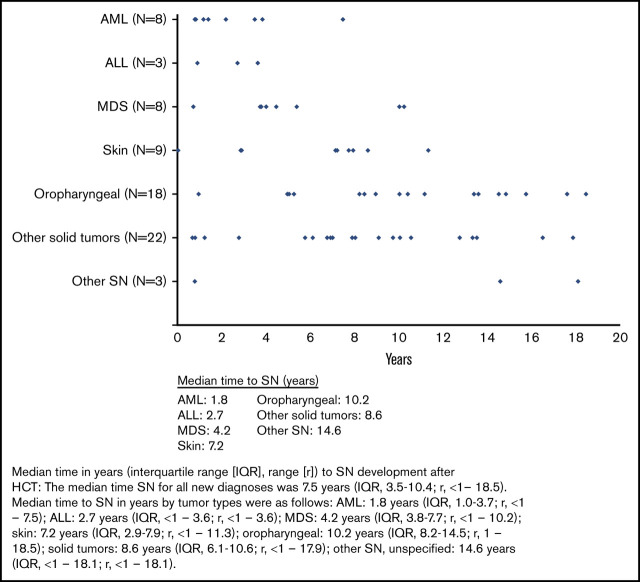
We examined the risk of subsequent neoplasms (SNs) and late mortality in children and adolescents undergoing allogeneic hematopoietic cell transplantation (HCT) for nonmalignant diseases (NMDs). We included 6028 patients (median age, 6 years; interquartile range, 1-11; range, <1 to 20) from the Center for International Blood and Marrow Transplant Research (1995-2012) registry. Standardized mortality ratios (SMRs) in 2-year survivors and standardized incidence ratios (SIRs) were calculated to compare mortality and SN rates with expected rates in the general population. Median follow-up of survivors was 7.8 years. Diagnoses included severe aplastic anemia (SAA; 24%), Fanconi anemia (FA; 10%), other marrow failure (6%), hemoglobinopathy (15%), immunodeficiency (23%), and metabolic/leukodystrophy syndrome (22%). Ten-year survival was 93% (95% confidence interval [95% CI], 92% to 94%; SMR, 4.2; 95% CI, 3.7-4.8). Seventy-one patients developed SNs (1.2%). Incidence was highest in FA (5.5%), SAA (1.1%), and other marrow failure syndromes (1.7%); for other NMDs, incidence was <1%. Hematologic (27%), oropharyngeal (25%), and skin cancers (13%) were most common. Leukemia risk was highest in the first 5 years posttransplantation; oropharyngeal, skin, liver, and thyroid tumors primarily occurred after 5 years. Despite a low number of SNs, patients had an 11-fold increased SN risk (SIR, 11; 95% CI, 8.9-13.9) compared with the general population. We report excellent long-term survival and low SN incidence in an international cohort of children undergoing HCT for NMDs. The risk of SN development was highest in patients with FA and marrow failure syndromes, highlighting the need for long-term posttransplantation surveillance in this population.
我们研究了接受异基因造血细胞移植(HCT)治疗非恶性疾病(NMD)的儿童和青少年发生后续肿瘤(SN)及晚期死亡的风险。我们纳入了国际血液和骨髓移植研究中心(1995 - 2012年)登记的6028例患者(中位年龄6岁;四分位间距1 - 11岁;范围<1至20岁)。计算了2年存活者的标准化死亡率(SMR)和标准化发病率(SIR),以比较死亡率和SN发生率与一般人群的预期率。存活者的中位随访时间为7.8年。诊断包括重型再生障碍性贫血(SAA;24%)、范可尼贫血(FA;10%)、其他骨髓衰竭(6%)、血红蛋白病(15%)、免疫缺陷(23%)以及代谢/脑白质营养不良综合征(22%)。10年生存率为93%(95%置信区间[95%CI],92%至94%;SMR,4.2;95%CI,3.7 - 4.8)。71例患者发生了SN(1.2%)。发病率在FA(5.5%)、SAA(1.1%)和其他骨髓衰竭综合征中最高(1.7%);对于其他NMD,发病率<1%。血液系统肿瘤(27%)、口咽肿瘤(25%)和皮肤癌(13%)最为常见。白血病风险在移植后前5年最高;口咽、皮肤、肝脏和甲状腺肿瘤主要发生在5年后。尽管SN数量较少,但与一般人群相比,患者发生SN的风险增加了11倍(SIR,11;95%CI,8.9 - 13.9)。我们报告了一组接受HCT治疗NMD的国际儿童队列具有出色的长期生存率和较低的SN发病率。FA和骨髓衰竭综合征患者发生SN的风险最高,突出了对该人群进行长期移植后监测的必要性。