Hospital Israelita Albert Einstein, São Paulo, SP, Brasil.
Hospital do Servidor Público Estadual "Francisco Morato de Oliveira", São Paulo, SP, Brasil.
Rev Bras Ter Intensiva. 2020 Mar;32(1):17-27. doi: 10.5935/0103-507x.20200005. Epub 2020 May 8.
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
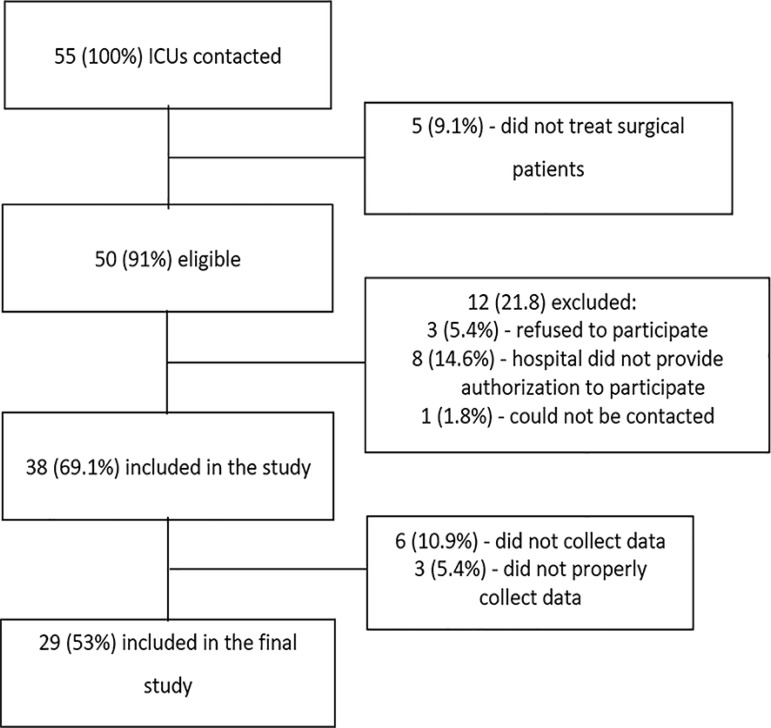
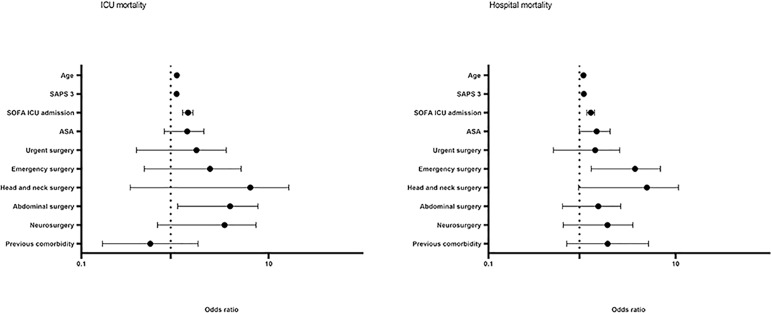
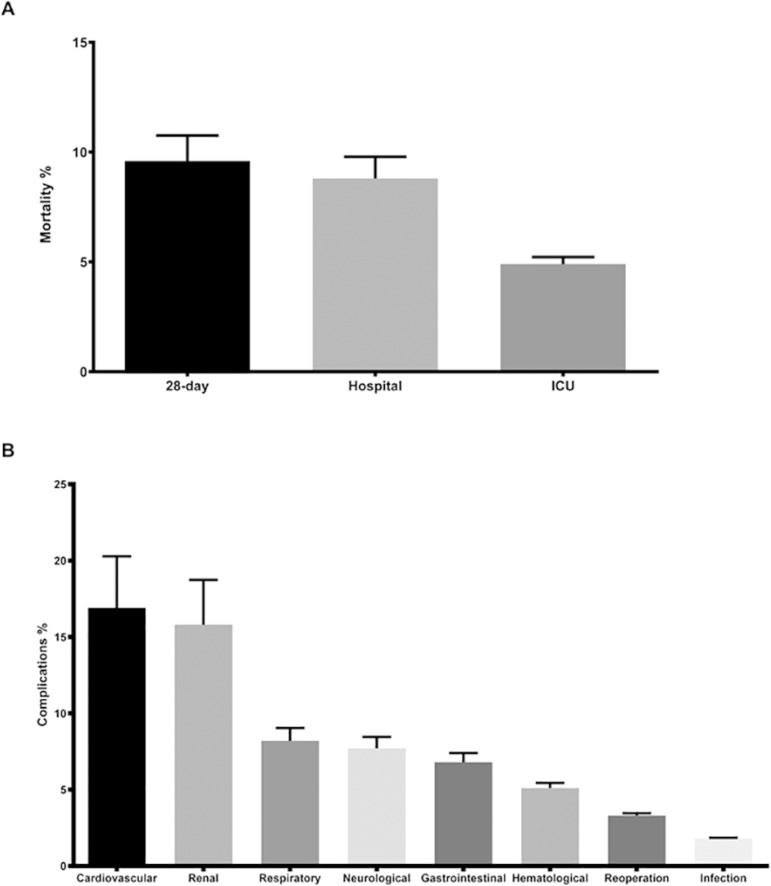
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval - 95%CI 3.3% - 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 - 4.0) days, and the length of hospital stay was 9.5 (5.4 - 18.6) days. The complication rate was 29.9% (95%CI 26.4 - 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 - 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio - OR = 1.02; 95%CI 1.01 - 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 - 1.25), surgical time (OR = 1.001, 95%CI 1.000 - 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 - 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 - 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 - 1.279), SOFA (OR = 1.175, 95%CI 1.069 - 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 - 6.051).
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
定义巴西非心脏高手术风险患者的流行病学特征和发病率及死亡率的主要决定因素。
这是一项前瞻性、观察性和多中心研究。在 1 个月内,所有被收入重症监护病房的非心脏手术患者,即被认为是高危患者,每天进行评估和监测,最多监测 7 天,以确定并发症。评估术后 28 天、重症监护病房和住院死亡率。
29 个重症监护病房参与了这项研究。共进行了 25500 例手术,其中 904 例(3.5%)为高危患者(95%置信区间[95%CI]3.3%-3.8%),并纳入了研究。参与患者中,48.3%来自私立重症监护病房,51.7%来自公立医院重症监护病房。重症监护病房的住院时间为 2.0(1.0-4.0)天,住院时间为 9.5(5.4-18.6)天。并发症发生率为 29.9%(95%CI 26.4%-33.7%),术后 28 天死亡率为 9.6%(95%CI 7.4%-12.1%)。并发症的独立危险因素是简化急性生理学评分 3(SAPS 3;优势比[OR]=1.02;95%CI 1.01-1.03)和重症监护病房入院时的序贯器官衰竭评估评分(SOFA)(OR=1.17;95%CI 1.09-1.25)、手术时间(OR=1.001,95%CI 1.000-1.002)和急诊手术(OR=1.93,95%CI,1.10-3.38)。此外,还与 28 天死亡率(OR=1.032;95%CI 1.011-1.052)、SAPS 3(OR=1.041;95%CI 1.107-1.279)、SOFA(OR=1.175,95%CI 1.069-1.292)和急诊手术(OR=2.509;95%CI 1.040-6.051)相关。
更高的预后评分、老年患者、较长的手术时间和急诊手术与 28 天死亡率更高和重症监护病房住院期间更多并发症密切相关。