Department of Biomedical Physiology and Kinesiology, Simon Fraser University, Burnaby, BC, Canada.
Department of Sports Science and Physical Education, The Chinese University of Hong Kong, Hong Kong, China.
J Bone Miner Res. 2020 Oct;35(10):1914-1922. doi: 10.1002/jbmr.4048. Epub 2020 Jul 6.
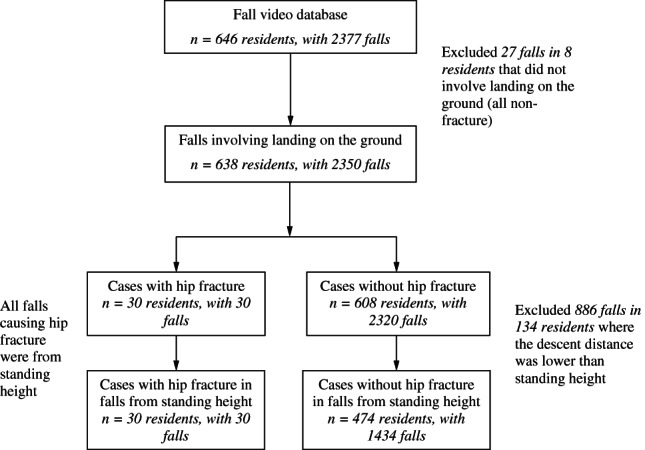
Over 95% of hip fractures in older adults are caused by falls, yet only 1% to 2% of falls result in hip fracture. Our current understanding of the types of falls that lead to hip fracture is based on reports by the faller or witness. We analyzed videos of real-life falls in long-term care to provide objective evidence on the factors that separate falls that result in hip fracture from falls that do not. Between 2007 and 2018, we video-captured 2377 falls by 646 residents in two long-term care facilities. Hip fracture was documented in 30 falls. We analyzed each video with a structured questionnaire, and used generalized estimating equations (GEEs) to determine relative risk ratios (RRs) for hip fracture associated with various fall characteristics. All hip fractures involved falls from standing height, and pelvis impact with the ground. After excluding falls from lower than standing height, risk for hip fracture was higher for sideways landing configurations (RR = 5.50; 95% CI, 2.36-12.78) than forward or backward, and for falls causing hip impact (3.38; 95% CI, 1.49-7.67). However, hip fracture risk was just as high in falls initially directed sideways as forward (1.14; 95% CI, 0.49-2.67), due to the tendency for rotation during descent. Falling while using a mobility aid was associated with lower fracture risk (0.30; 95% CI, 0.09-1.00). Seventy percent of hip fractures involved impact to the posterolateral aspect of the pelvis. Hip protectors were worn in 73% of falls, and hip fracture risk was lower in falls where hip protectors were worn (0.45; 95% CI, 0.21-0.99). Age and sex were not associated with fracture risk. There was no evidence of spontaneous fractures. In this first study of video-captured falls causing hip fracture, we show that the biomechanics of falls involving hip fracture were different than nonfracture falls for fall height, fall direction, impact locations, and use of hip protectors. © 2020 The Authors. Journal of Bone and Mineral Research published by American Society for Bone and Mineral Research.
超过 95%的老年人髋部骨折是由跌倒引起的,但只有 1%到 2%的跌倒会导致髋部骨折。我们目前对导致髋部骨折的跌倒类型的了解是基于跌倒者或目击者的报告。我们分析了长期护理中真实跌倒的视频,以提供关于将导致髋部骨折的跌倒与不导致髋部骨折的跌倒区分开来的因素的客观证据。在 2007 年至 2018 年期间,我们在两家长期护理机构对 646 名居民的 2377 次跌倒进行了视频拍摄。30 次跌倒导致髋部骨折。我们使用结构化问卷对每个视频进行了分析,并使用广义估计方程(GEE)确定与各种跌倒特征相关的髋部骨折的相对风险比(RR)。所有髋部骨折均涉及站立高度的跌倒,以及骨盆与地面的撞击。在排除低于站立高度的跌倒后,侧向着地配置(RR = 5.50;95%CI,2.36-12.78)比前向或后向着地以及导致髋部撞击的跌倒(3.38;95%CI,1.49-7.67)的髋部骨折风险更高。然而,由于下降过程中的旋转趋势,最初侧向跌倒的髋部骨折风险与向前跌倒一样高(1.14;95%CI,0.49-2.67)。使用助行器时跌倒与较低的骨折风险相关(0.30;95%CI,0.09-1.00)。70%的髋部骨折涉及骨盆的后外侧撞击。73%的跌倒中佩戴了髋部保护器,佩戴髋部保护器的跌倒中髋部骨折风险较低(0.45;95%CI,0.21-0.99)。年龄和性别与骨折风险无关。没有自发性骨折的证据。在这项关于导致髋部骨折的视频拍摄跌倒的首次研究中,我们表明涉及髋部骨折的跌倒的生物力学与非骨折跌倒在跌倒高度、跌倒方向、撞击位置和髋部保护器的使用方面有所不同。