Department of Urology, The First Affiliated Hospital of Nanchang University, Nanchang, China.
Department of Anesthesiology, The First Affiliated Hospital of Nanchang University, Nanchang, China.
BJU Int. 2020 Aug;126(2):300-308. doi: 10.1111/bju.15111. Epub 2020 Jun 1.
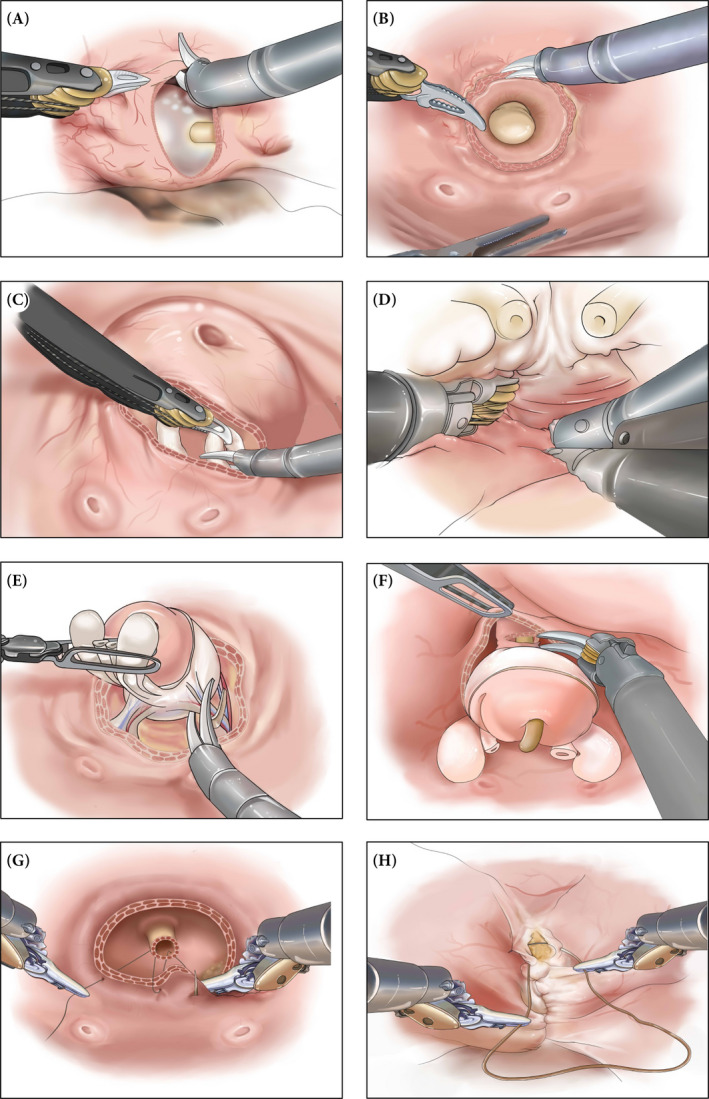
To describe in detail the techniques for transvesical robot-assisted radical prostatectomy (RARP) using the da Vinci Si/Xi system (Intuitive Surgical, Sunnyvale, CA, USA) and to evaluate functional and oncological outcomes in 35 patients with prostate cancer.
Thirty-five patients with localized prostate cancer were enrolled for transvesical RARP. The patients' preoperative data (mean ± sd age 63.4 ± 8.1 years, body mass index 28.6 ± 5.3 kg/m , total prostate-specific antigen 10.8 ± 4.9 ng/mL and prostate volume 30.6 ± 14.4 mL, and median [interquartile range {IQR}] biopsy Gleason score 6 [6-7], and International Index of Erectile Function [IIEF]-5 score 18 [16-20]) were collected. Preoperative assessment revealed 28 cases of cT2a and seven cases of cT2b disease. All patients were continent preoperatively (defined as no pad required or one dry pad per day as a precaution). Surgical results and peri-operative complications were assessed. All patients were followed up for at least 12 months postoperatively.
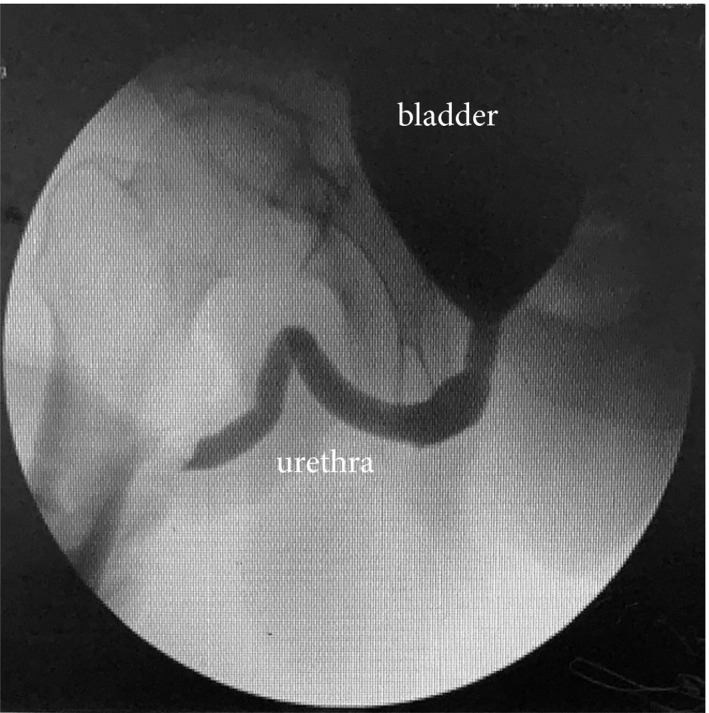
The mean operating time was 150 ± 35 min. Estimated blood loss was 100 ± 45 mL. Urinary infection was noted in one patient and managed with levofloxacin. Another patient complained of nocturia on postoperative day 14, which was relieved with solifenacin succinate. Urethral catheters were removed on postoperative day 7. Thirty-two patients achieved immediate urinary continence, with three patients returning to full continence on postoperative day 14. Postoperative pathology confirmed 24 pT2a cases, nine pT2b cases and two pT2c cases (median [IQR] Gleason score 6 [6-7]). Positive surgical margins were found in four patients (11.4%). No urethral stricture or urinary leakage was noted on urethrocystography taken 3 months after surgery. Urodynamic studies were performed preoperatively and 6 months after surgery: median (IQR) maximum urinary flow 12.2 (10.2-14.9) vs 13.7 (10.1-15.0) mL/s; bladder capacity 385.3 (351.3-410.2) vs 370.2 (330.1-395.4) mL; and voiding phase detrusor contractility 38.5 (27.8-42.3) vs 35.6 (28.3-41.3) mmH O, respectively. During a minimum of 12 months of follow-up, no biochemical recurrence was noted in any patient. The median (IQR) IIEF-5 score was 17 (16-19).
The transvesical approach is a valid alternative to RARP in selected patients, providing promising postoperative urinary continence. Long-term functional and oncological results require further investigation.
详细描述使用达芬奇 Si/Xi 系统(直观外科公司,加利福尼亚州森尼韦尔)进行经膀胱机器人辅助根治性前列腺切除术(RARP)的技术,并评估 35 例前列腺癌患者的功能和肿瘤学结果。
35 例局限性前列腺癌患者接受经膀胱 RARP 治疗。收集患者的术前数据(平均±标准差年龄 63.4±8.1 岁,体重指数 28.6±5.3kg/m ,总前列腺特异性抗原 10.8±4.9ng/ml 和前列腺体积 30.6±14.4ml,中位[四分位距{IQR}]活检 Gleason 评分 6[6-7],国际勃起功能指数[IIEF]-5 评分 18[16-20])。术前评估显示 28 例 cT2a 期和 7 例 cT2b 期疾病。所有患者术前均有控尿能力(定义为无需使用尿垫或每天使用一片尿垫作为预防措施)。评估手术结果和围手术期并发症。所有患者术后至少随访 12 个月。
平均手术时间为 150±35 分钟。估计失血量为 100±45ml。1 例患者发生尿路感染,给予左氧氟沙星治疗。另 1 例患者术后 14 天出现夜尿,给予琥珀酸索利那新缓解。术后第 7 天拔除尿道导管。32 例患者立即获得尿控,3 例患者术后 14 天恢复完全尿控。术后病理证实 24 例 pT2a 期、9 例 pT2b 期和 2 例 pT2c 期(中位[IQR]Gleason 评分 6[6-7])。4 例患者(11.4%)发现阳性切缘。术后 3 个月行尿道膀胱造影未见尿道狭窄或尿漏。术前和术后 6 个月行尿动力学检查:最大尿流率中位数(IQR)分别为 12.2(10.2-14.9)和 13.7(10.1-15.0)ml/s;膀胱容量中位数(IQR)分别为 385.3(351.3-410.2)和 370.2(330.1-395.4)ml;逼尿肌收缩期逼尿肌收缩力中位数(IQR)分别为 38.5(27.8-42.3)和 35.6(28.3-41.3)mmHg。在至少 12 个月的随访中,无患者出现生化复发。中位(IQR)IIEF-5 评分为 17(16-19)。
经膀胱入路是一种有选择地应用于 RARP 的有效替代方法,可为患者提供有希望的术后尿控。长期的功能和肿瘤学结果需要进一步研究。