Martin-Fernandez Marta, Bravo García-Morato María, Gruber Conor, Murias Loza Sara, Malik Muhammad Nasir Hayat, Alsohime Fahad, Alakeel Abdullah, Valdez Rita, Buta Sofija, Buda Guadalupe, Marti Marcelo A, Larralde Margarita, Boisson Bertrand, Feito Rodriguez Marta, Qiu Xueer, Chrabieh Maya, Al Ayed Mohammed, Al Muhsen Saleh, Desai Jigar V, Ferre Elise M N, Rosenzweig Sergio D, Amador-Borrero Blanca, Bravo-Gallego Luz Yadira, Olmer Ruth, Merkert Sylvia, Bret Montserrat, Sood Amika K, Al-Rabiaah Abdulkarim, Temsah Mohamad Hani, Halwani Rabih, Hernandez Michelle, Pessler Frank, Casanova Jean-Laurent, Bustamante Jacinta, Lionakis Michail S, Bogunovic Dusan
Department of Microbiology, Icahn School of Medicine at Mount Sinai, New York, NY 10029, USA; Department of Pediatrics, Icahn School of Medicine at Mount Sinai, New York, NY 10029, USA; The Mindich Child Health and Development Institute, Icahn School of Medicine at Mount Sinai, New York, NY 10029, USA.
Hospital Universitario La Paz, 28046 Madrid, Spain.
Cell Rep. 2020 May 12;31(6):107633. doi: 10.1016/j.celrep.2020.107633.
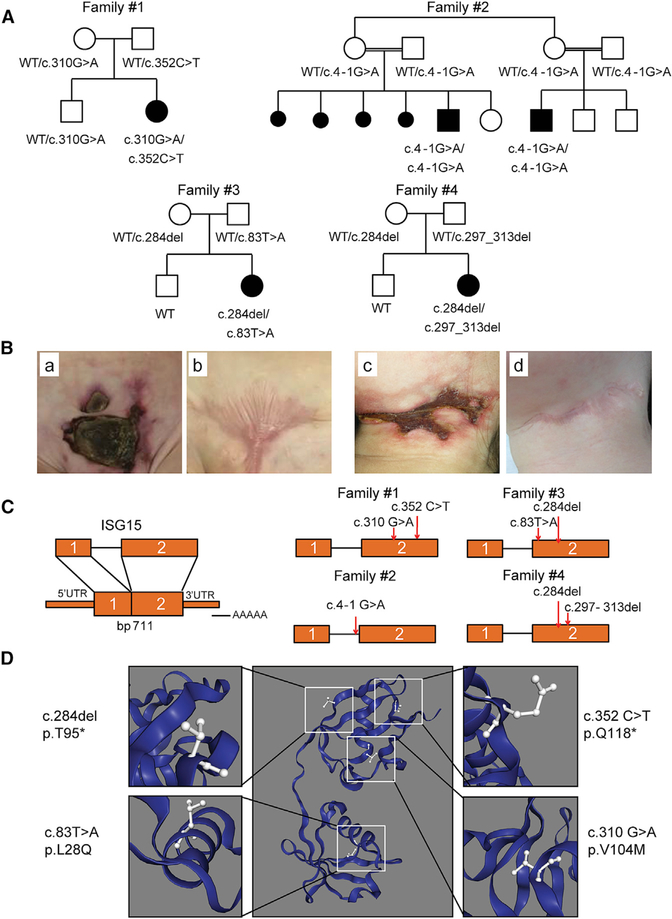
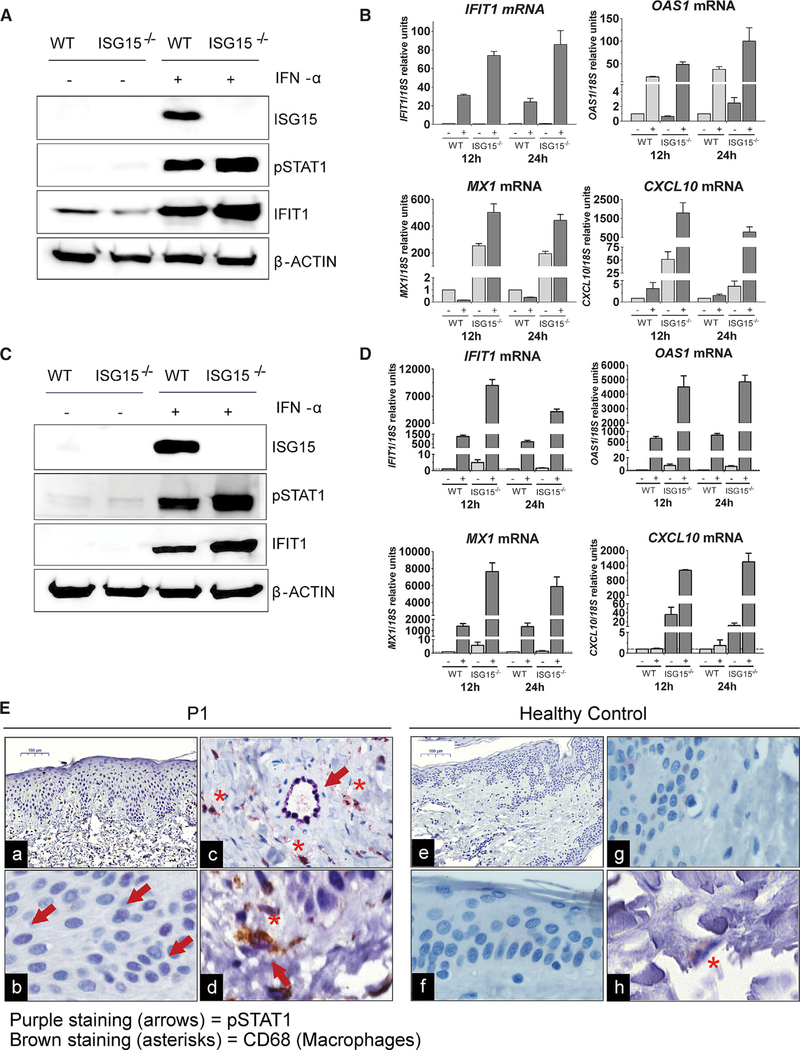
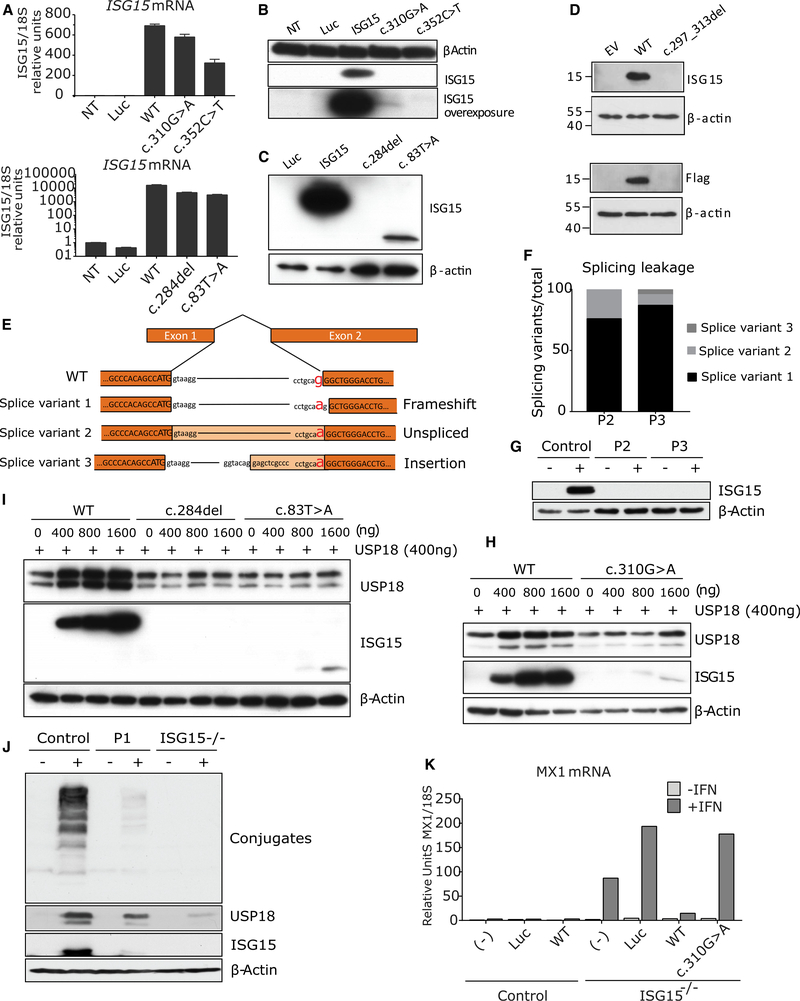
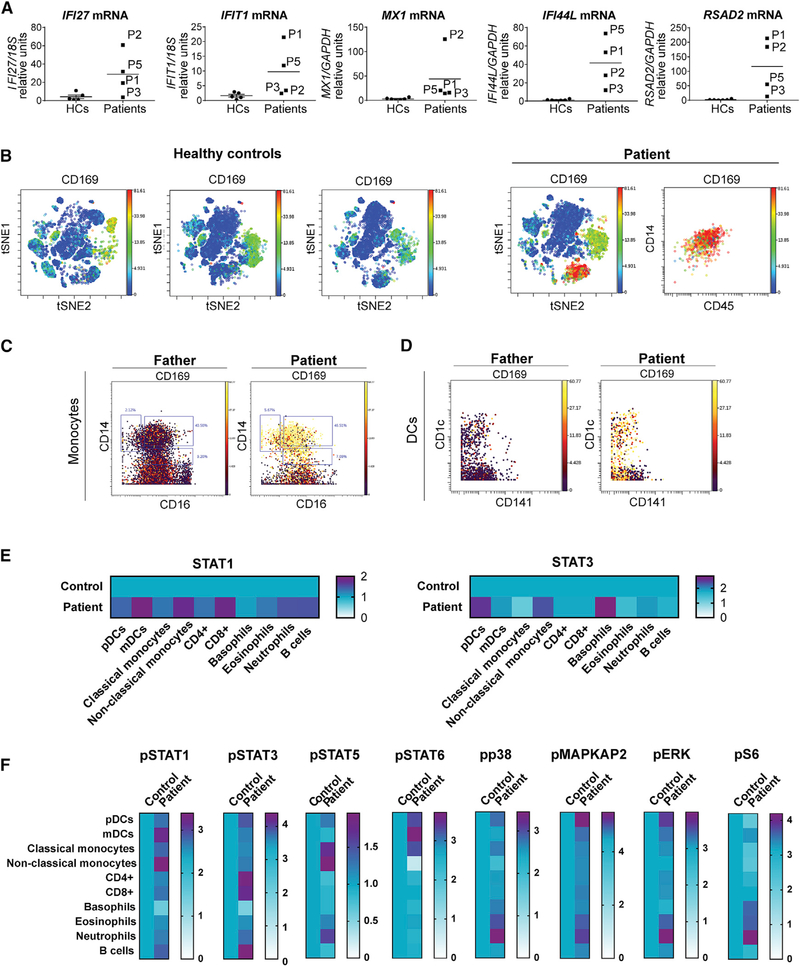
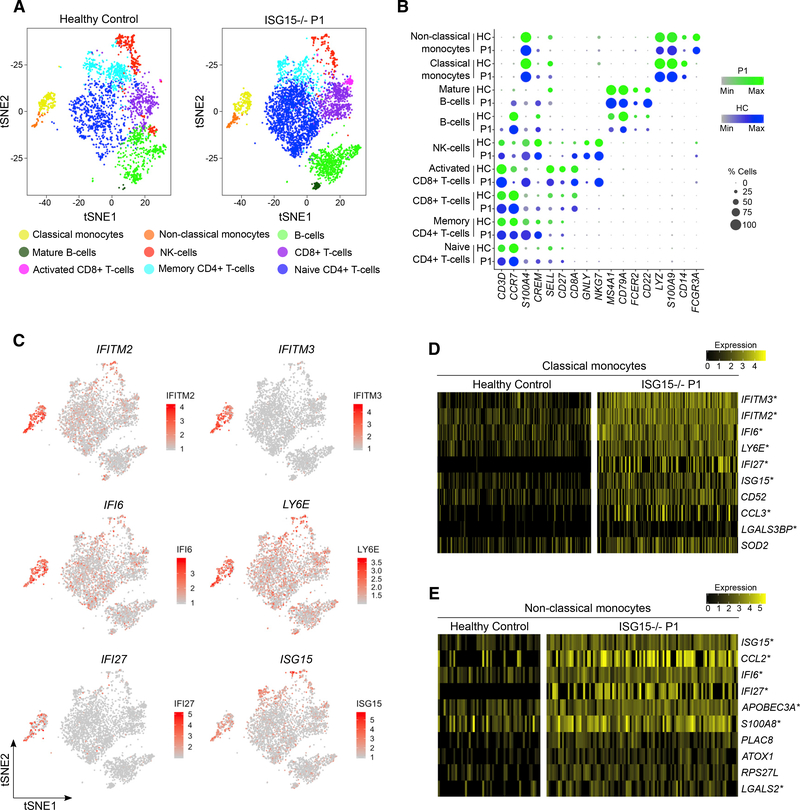
Most monogenic disorders have a primary clinical presentation. Inherited ISG15 deficiency, however, has manifested with two distinct presentations to date: susceptibility to mycobacterial disease and intracranial calcifications from hypomorphic interferon-II (IFN-II) production and excessive IFN-I response, respectively. Accordingly, these patients were managed for their infectious and neurologic complications. Herein, we describe five new patients with six novel ISG15 mutations presenting with skin lesions who were managed for dermatologic disease. Cellularly, we denote striking specificity to the IFN-I response, which was previously assumed to be universal. In peripheral blood, myeloid cells display the most robust IFN-I signatures. In the affected skin, IFN-I signaling is observed in the keratinocytes of the epidermis, endothelia, and the monocytes and macrophages of the dermis. These findings define the specific cells causing circulating and dermatologic inflammation and expand the clinical spectrum of ISG15 deficiency to dermatologic presentations as a third phenotype co-dominant to the infectious and neurologic manifestations.
大多数单基因疾病都有主要的临床表现。然而,迄今为止,遗传性ISG15缺乏症已表现出两种不同的症状:分别是对分枝杆菌病的易感性以及因低水平干扰素-II(IFN-II)产生和过度IFN-I反应导致的颅内钙化。因此,这些患者针对其感染性和神经系统并发症进行了治疗。在此,我们描述了五名新患者,他们携带六个新的ISG15突变,表现为皮肤病变,并针对皮肤病进行了治疗。在细胞层面,我们发现对IFN-I反应具有显著的特异性,而此前认为这种反应是普遍存在的。在外周血中,髓样细胞表现出最强的IFN-I信号特征。在受影响的皮肤中,在表皮的角质形成细胞、内皮细胞以及真皮的单核细胞和巨噬细胞中观察到IFN-I信号传导。这些发现确定了导致循环和皮肤炎症的特定细胞,并将ISG15缺乏症的临床谱扩展到皮肤表现,作为与感染性和神经学表现共同占主导地位的第三种表型。