RAND Corporation, Santa Monica, CA, USA.
Office of Public Health Studies, University of Hawaii, Honolulu, HI, USA.
BMC Musculoskelet Disord. 2020 May 13;21(1):298. doi: 10.1186/s12891-020-03330-1.
Chronic spinal pain is prevalent, expensive and long-lasting. Several provider-based nonpharmacologic therapies have now been recommended for chronic low-back pain (CLBP) and chronic neck pain (CNP). However, healthcare and coverage policies provide little guidance or evidence regarding the long-term use of this care. To provide one glimpse into the long-term use of nonpharmacologic provider-based care, this study examines the predictors of visit frequency in a large sample of patients with CLBP and CNP using ongoing chiropractic care.
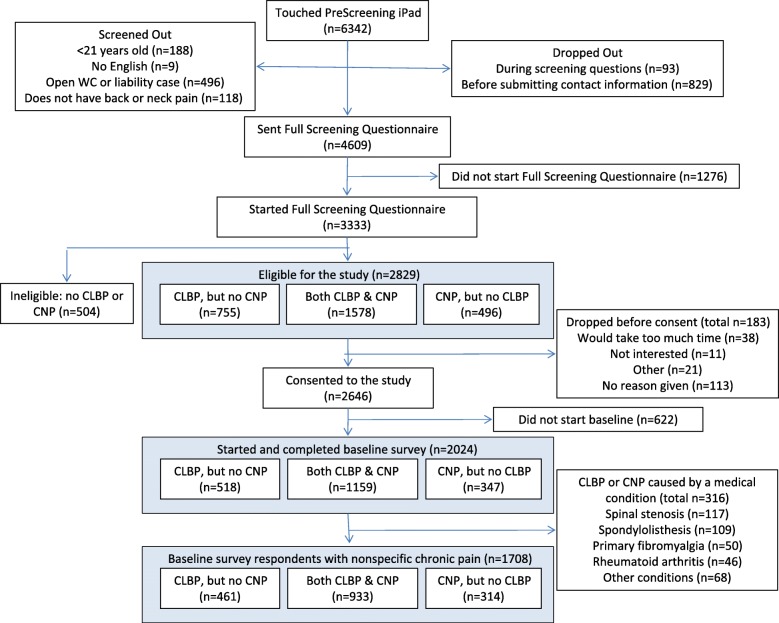
Observational data were collected from a large national sample of chiropractic patients in the US with non-specific CLBP and CNP. Visit frequency was defined as average number of chiropractic visits per month over the 3-month study period. Potential baseline predictor variables were entered into two sets of multi-level models according to a defined causal theory-in this case, Anderson's Behavioral Model of Health Services Use.
Our sample included 852 patients with CLBP and 705 with CNP. Visit frequency varied significantly by chiropractor/clinic, so our models controlled for this clustering. Patients with either condition used an average of 2.3 visits per month. In the final models visit frequency increased (0.44 visits per month, p = .008) for those with CLBP and some coverage for chiropractic, but coverage had little effect on visits for patients with CNP. Patients with worse function or just starting care also had more visits and those near to ending care had fewer visits. However, visit frequency was also determined by the chiropractor/clinic where treatment was received. Chiropractors who reported seeing more patients per day also had patients with higher visit frequency, and the patients of chiropractors with 20 to 30 years of experience had fewer visits per month. In addition, after controlling for both patient and chiropractor characteristics, the state in which care was received made a difference, likely through state-level policies and regulations.
Chiropractic patients with CLBP and CNP use a range of visit frequencies for their ongoing care. The predictors of these frequencies could be useful for understanding and developing policies for ongoing provider-based care.
慢性脊柱疼痛普遍存在、代价高昂且持续时间长。目前已推荐几种基于提供者的非药物疗法用于慢性下腰痛(CLBP)和慢性颈痛(CNP)。然而,医疗保健和覆盖政策几乎没有提供关于这种护理的长期使用的指导或证据。为了提供对非药物提供者为基础的护理的长期使用的一个视角,本研究使用持续的整脊治疗,在一个有大量 CLBP 和 CNP 患者的样本中检查了就诊频率的预测因素。
本研究从美国的一个大型全国性整脊患者样本中收集了非特异性 CLBP 和 CNP 的观察性数据。就诊频率定义为研究期间每 3 个月的平均就诊次数。根据已确定的因果理论(即安德森健康服务使用行为模型),将潜在的基线预测变量输入两组多水平模型中。
我们的样本包括 852 例 CLBP 患者和 705 例 CNP 患者。就诊频率因整脊医生/诊所而异,因此我们的模型控制了这种聚类。患有任何一种疾病的患者平均每月就诊 2.3 次。在最终模型中,CLBP 患者的就诊频率增加(每月增加 0.44 次,p=0.008),并且有一些覆盖整脊治疗的保险,但对 CNP 患者的就诊次数影响不大。功能较差或刚开始治疗的患者就诊次数更多,接近结束治疗的患者就诊次数更少。然而,就诊频率也取决于接受治疗的整脊医生/诊所。报告每天看诊更多患者的整脊医生也有就诊频率更高的患者,并且有 20 至 30 年经验的整脊医生的患者每月就诊次数更少。此外,在控制了患者和整脊医生的特征后,护理的所在州也有所不同,这可能是通过州级政策和法规实现的。
患有 CLBP 和 CNP 的整脊患者对其持续护理的就诊频率范围不同。这些频率的预测因素对于理解和制定持续提供者为基础的护理政策可能有用。