Department of Global Health, Save the Children, Washington, DC, 20002, USA.
Center for Global Health. US Centers for Disease Control and Prevention, 1600 Clifton Rd, Atlanta, GA, 30329-4027, USA.
BMC Pediatr. 2020 May 13;20(1):215. doi: 10.1186/s12887-020-02120-x.
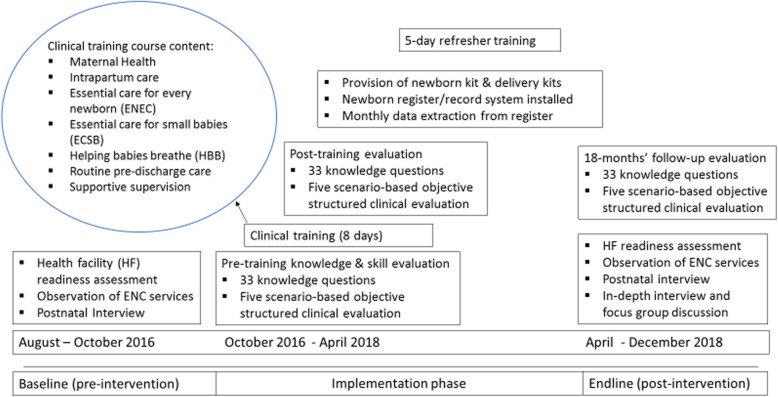
Increasingly, neonatal mortality is concentrated in settings of conflict and political instability. To promote evidence-based practices, an interagency collaboration developed the Newborn Health in Humanitarian Settings: Field Guide. The essential newborn care component of the Field Guide was operationalized with the use of an intervention package encompassing the training of health workers, newborn kit provisions and the installation of a newborn register.
We conducted a quasi-experimental prepost study to test the effectiveness of the intervention package on the composite outcome of essential newborn care from August 2016 to December 2018 in Bossaso, Somalia. Data from the observation of essential newborn care practices, evaluation of providers' knowledge and skills, postnatal interviews, and qualitative information were analyzed. Differences in two-proportion z-tests were used to estimate change in essential newborn care practices. A generalized estimating equation was applied to account for clustering of practice at the health facility level.
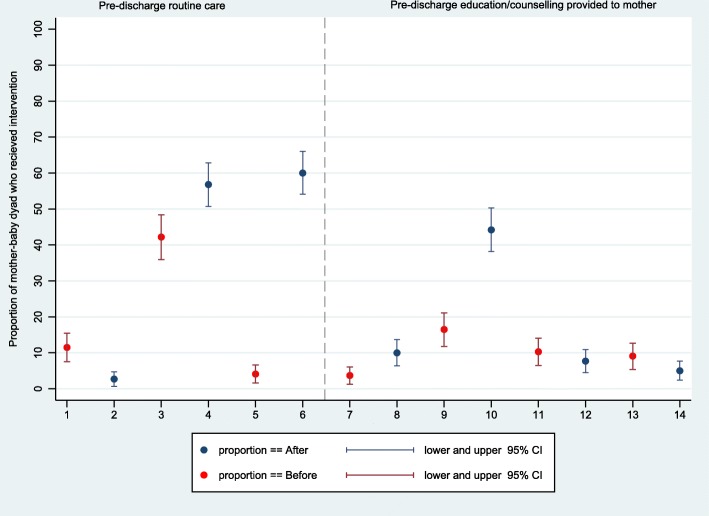
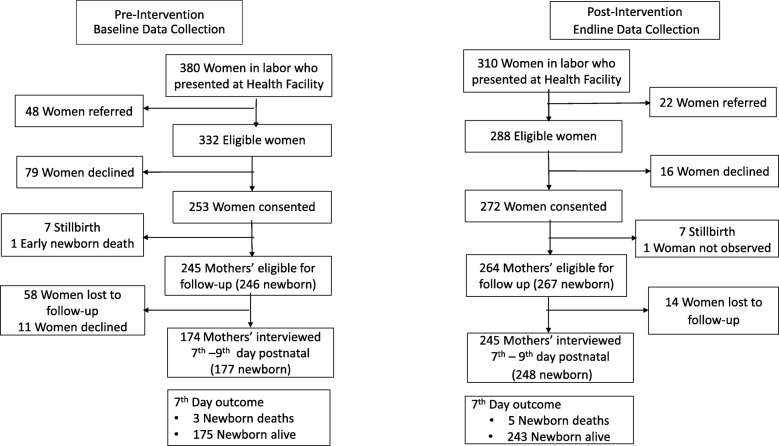
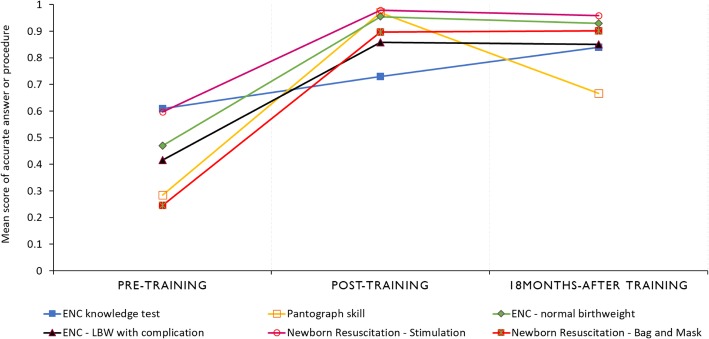
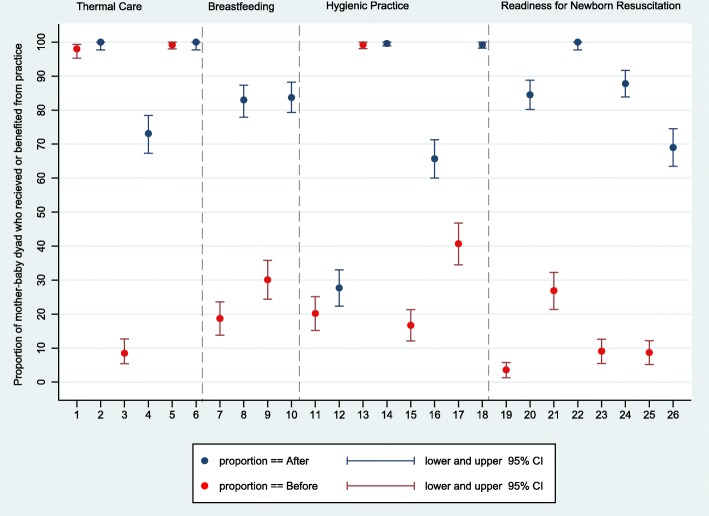
Among the 690 pregnant women in labor who sought care at the health facilities, 89.9% (n = 620) were eligible for inclusion, 84.7% (n = 525) were enrolled, and newborn outcomes were ascertained in 79.8% (n = 419). Providers' knowledge improved from pre to posttraining, with a mean difference in score of + 11.9% (95% CI: 7.2, 16.6, p-value < 0.001) and from posttraining to 18-months after training with a mean difference of + 10.9% (95% CI: 4.7, 17.0, p-value < 0.001). The proportion of newborns who received two or more essential newborn care practices (skin-to-skin contact, early breastfeeding, and dry cord care) improved from 19.9% (95% CI: 4.9, 39.7) to 94.7% (95% CI: 87.7, 100.0). In the adjusted model that accounted for clustering at health facilities, the odds of receiving two or more essential newborn practices was 64.5 (95% CI: 15.8, 262.6, p-value < 0.001) postintervention compared to preintervention. Predischarge education offered to mothers on breastfeeding 16.5% (95% CI: 11.8, 21.1) vs 44.2% (95% CI: 38.2, 50.3) and newborn illness danger signs 9.1% (95% CI: 5.4, 12.7) vs 5.0% (95% CI: 2.4, 7.7) remained suboptimal.
The intervention package was feasible and effective in improving essential newborn care. Knowledge and skills gained after training were mostly retained at the 18-month follow-up.
越来越多的新生儿死亡集中在冲突和政治不稳定的环境中。为了促进循证实践,一个机构间合作组织制定了《人道主义环境中的新生儿健康:现场指南》。该指南的基本新生儿护理部分通过使用涵盖卫生工作者培训、新生儿包供应和新生儿登记册安装的干预包来实施。
我们进行了一项准实验前后研究,以测试 2016 年 8 月至 2018 年 12 月在索马里博萨索干预包对基本新生儿护理综合结局的有效性。分析了基本新生儿护理实践观察、提供者知识和技能评估、产后访谈以及定性信息的数据。使用两比例 z 检验估计基本新生儿护理实践的变化。应用广义估计方程来解释卫生设施层面实践的聚类。
在寻求卫生设施分娩护理的 690 名孕妇中,89.9%(n=620)符合纳入条件,84.7%(n=525)入组,79.8%(n=419)确定了新生儿结局。提供者的知识在培训前后有所提高,平均分数提高了+11.9%(95%CI:7.2,16.6,p 值<0.001),培训后 18 个月提高了+10.9%(95%CI:4.7,17.0,p 值<0.001)。接受两种或两种以上基本新生儿护理措施(皮肤接触、早期母乳喂养和干燥脐带护理)的新生儿比例从 19.9%(95%CI:4.9,39.7)提高到 94.7%(95%CI:87.7,100.0)。在考虑卫生设施聚类的调整模型中,与干预前相比,接受两种或两种以上基本新生儿护理措施的可能性为 64.5(95%CI:15.8,262.6,p 值<0.001)。在出院前向母亲提供的母乳喂养教育为 16.5%(95%CI:11.8,21.1),新生儿疾病危险信号为 9.1%(95%CI:5.4,12.7),低于 44.2%(95%CI:38.2,50.3)和 5.0%(95%CI:2.4,7.7)。
该干预包是可行且有效的,能够改善基本新生儿护理。培训后获得的知识和技能在 18 个月的随访中大多得以保留。