Department of Internal Medicine, Section of Cardiovascular Medicine (M.G., V.S.R., J.F., D.M., C.M., T.A., D.J., L.B., J.M.T.), Yale University School of Medicine, New Haven, CT.
Hospital de Cardiologia, Instituto Mexicano del Seguro Social, Mexico City, Mexico (J.I.-M.).
Circulation. 2020 Sep 15;142(11):1028-1039. doi: 10.1161/CIRCULATIONAHA.120.045691. Epub 2020 May 15.
Sodium-glucose cotransporter-2 inhibitors improve heart failure-related outcomes. The mechanisms underlying these benefits are not well understood, but diuretic properties may contribute. Traditional diuretics such as furosemide induce substantial neurohormonal activation, contributing to the limited improvement in intravascular volume often seen with these agents. However, the proximal tubular site of action of the sodium-glucose cotransporter-2 inhibitors may help circumvent these limitations.
Twenty patients with type 2 diabetes mellitus and chronic, stable heart failure completed a randomized, placebo-controlled crossover study of empagliflozin 10 mg daily versus placebo. Patients underwent an intensive 6-hour biospecimen collection and cardiorenal phenotyping at baseline and again after 14 days of study drug. After a 2-week washout, patients crossed over to the alternate therapy with the above protocol repeated.
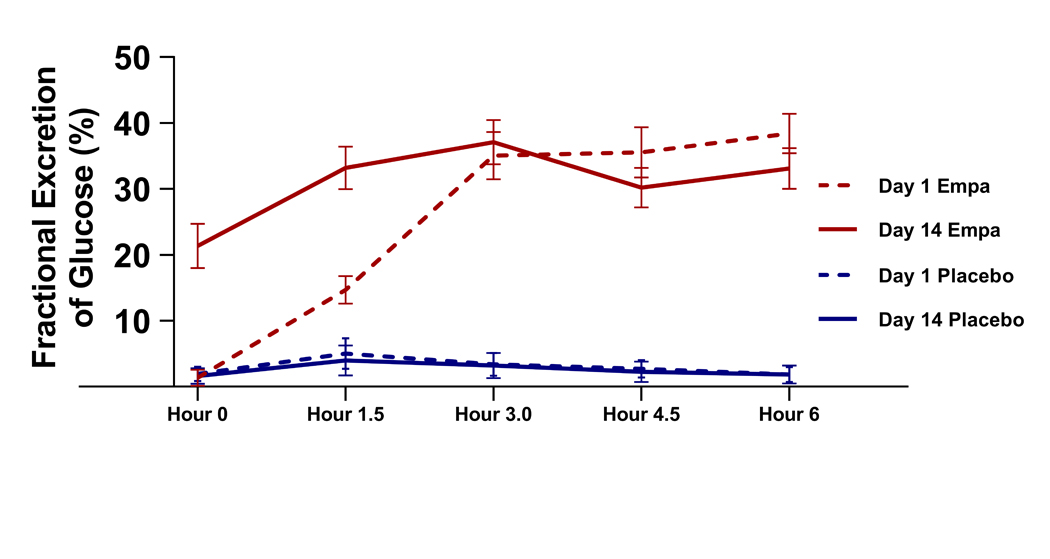
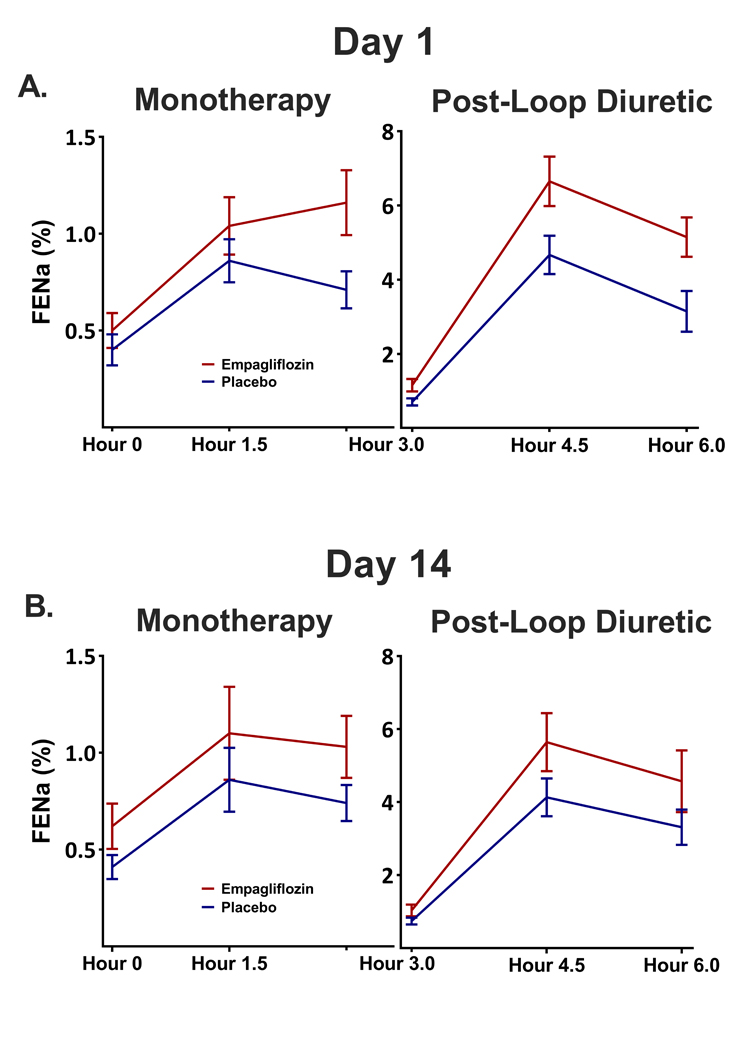
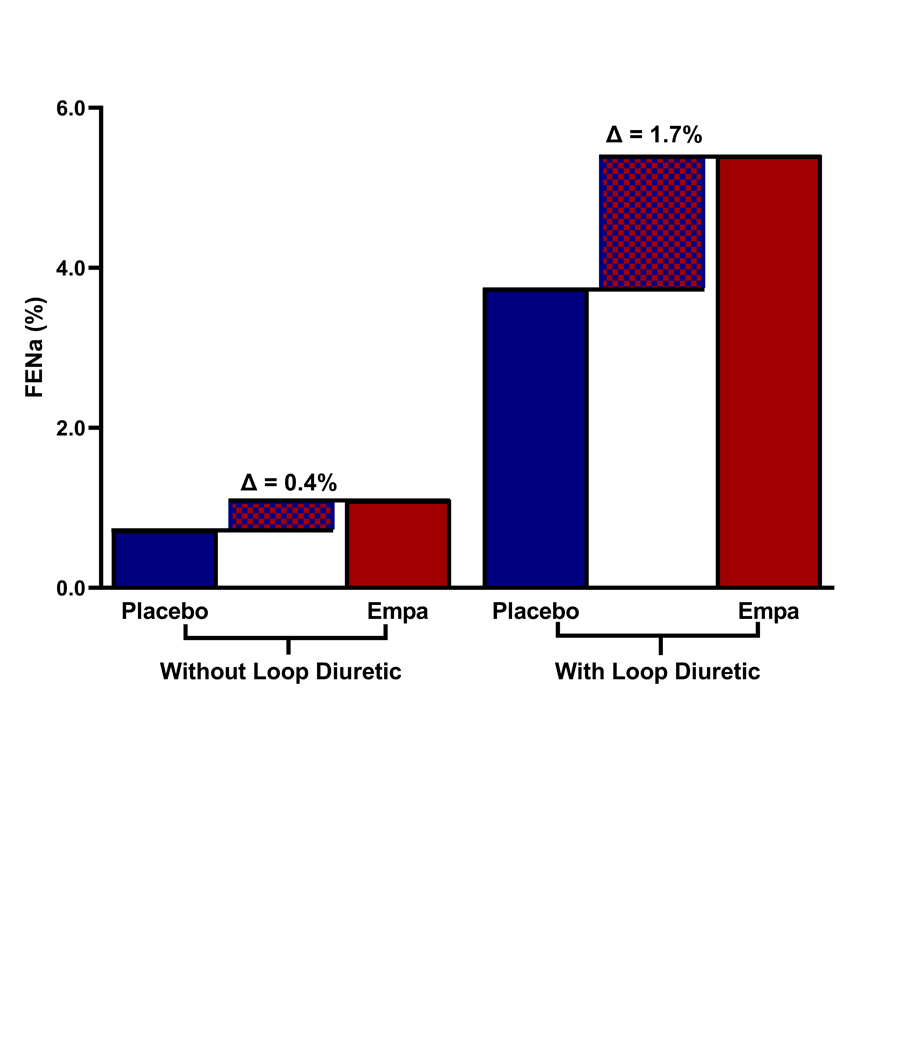
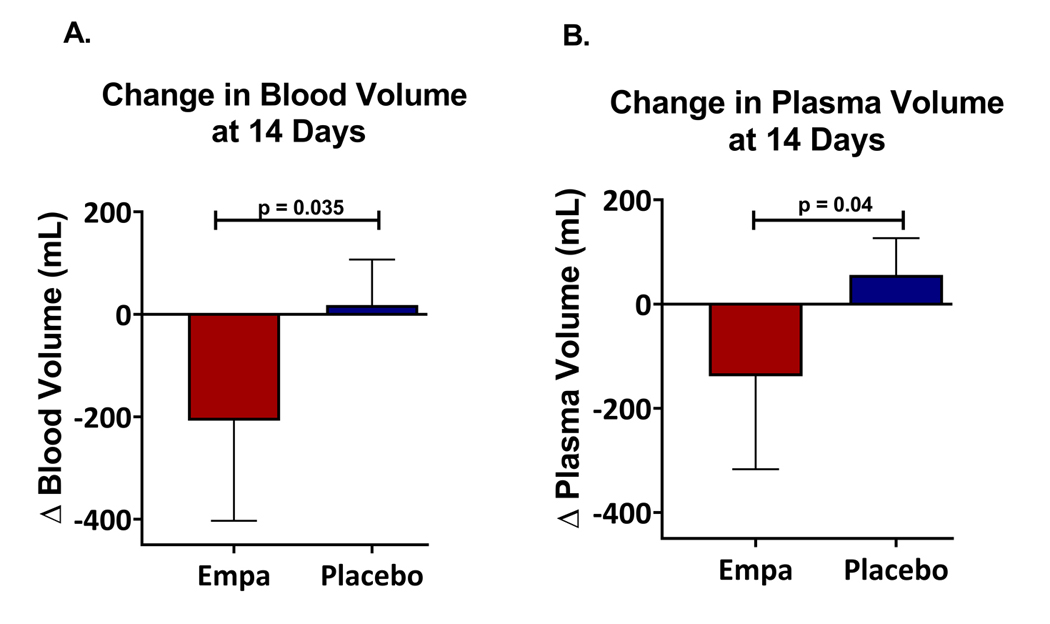
Oral empagliflozin was rapidly absorbed as evidenced by a 27-fold increase in urinary glucose excretion by 3 hours (<0.0001). Fractional excretion of sodium increased significantly with empagliflozin monotherapy versus placebo (fractional excretion of sodium, 1.2±0.7% versus 0.7±0.4%; =0.001), and there was a synergistic effect in combination with bumetanide (fractional excretion of sodium, 5.8±2.5% versus 3.9±1.9%; =0.001). At 14 days, the natriuretic effect of empagliflozin persisted, resulting in a reduction in blood volume (-208 mL [interquartile range, -536 to 153 mL] versus -14 mL [interquartile range, -282 to 335 mL]; =0.035) and plasma volume (-138 mL, interquartile range, -379 to 154±453 mL; =0.04). This natriuresis was not, however, associated with evidence of neurohormonal activation because the change in norepinephrine was superior (=0.02) and all other neurohormones were similar (<0.34) during the empagliflozin versus placebo period. Furthermore, there was no evidence of potassium wasting (=0.20) or renal dysfunction (>0.11 for all biomarkers), whereas both serum magnesium (<0.001) and uric acid levels (=0.008) improved.
Empagliflozin causes significant natriuresis, particularly when combined with loop diuretics, resulting in an improvement in blood volume. However, off-target electrolyte wasting, renal dysfunction, and neurohormonal activation were not observed. This favorable diuretic profile may offer significant advantage in the management of volume status in patients with heart failure and may represent a mechanism contributing to the superior long-term heart failure outcomes observed with these agents. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT03027960.
钠-葡萄糖共转运蛋白 2 抑制剂可改善心力衰竭相关结局。这些益处的潜在机制尚未完全明确,但利尿剂特性可能起到一定作用。传统利尿剂如呋塞米可引起显著的神经激素激活,这导致此类药物往往仅能有限地改善血管内容量。然而,钠-葡萄糖共转运蛋白 2 抑制剂的近端肾小管作用部位可能有助于规避这些局限性。
20 例患有 2 型糖尿病和慢性稳定型心力衰竭的患者完成了一项恩格列净 10mg 每日与安慰剂的随机、安慰剂对照交叉研究。患者在基线时和研究药物治疗 14 天后接受了强化 6 小时生物标本采集和心肾表型研究。在 2 周洗脱期后,患者交叉至另一治疗方案,并重复上述方案。
口服恩格列净迅速被吸收,证据为 3 小时内尿葡萄糖排泄增加了 27 倍(<0.0001)。与安慰剂相比,恩格列净单药治疗时钠的分数排泄显著增加(钠分数排泄,1.2±0.7%对 0.7±0.4%;=0.001),与布美他尼联合使用时具有协同作用(钠分数排泄,5.8±2.5%对 3.9±1.9%;=0.001)。在第 14 天,恩格列净的利尿作用持续存在,导致血容量减少(-208mL[四分位距(IQR),-536 至 153mL]对-14mL[IQR,-282 至 335mL];=0.035)和血浆容量减少(-138mL,IQR,-379 至 154±453mL;=0.04)。然而,这种利尿作用并未导致神经激素激活的证据,因为去甲肾上腺素的变化更优(=0.02),并且在恩格列净与安慰剂期间,所有其他神经激素均相似(<0.34)。此外,没有证据表明钾的丢失(=0.20)或肾功能障碍(所有生物标志物>0.11),而血清镁(<0.001)和尿酸水平(=0.008)均有所改善。
恩格列净可显著利尿,特别是与袢利尿剂联合使用时,可改善血容量。然而,未观察到非靶标电解质丢失、肾功能障碍和神经激素激活。这种有利的利尿特征可能在心力衰竭患者的容量状态管理方面具有显著优势,并可能代表这些药物在观察到的长期心力衰竭结局方面具有优势的一种机制。