Mo Liyi, Xie Zhen, Liu Guohui, He Qiang, Mo Zhiming, Wu Yanhua, Wang Wenji, Ding Feng, Liao Yuanjiang, Hao Li, Lu Chen, Sun Jin, Xu Libin, Zhang Yusheng, Ghappar Rizwangul, Peng Hongwei, Wei Xiaohong, Xie Jinglie, Chen Yuanhan, Liang Xinling
Division of Nephrology, Guangdong Provincial People's Hospital, Guangdong Academy of Medical Sciences, No.106 Zhongshan Road 2, Guangzhou, 510080, Guangdong, China.
Department of Nephrology, Dongguan People's Hospital, Dongguan, 523018, China.
BMC Health Serv Res. 2020 May 18;20(1):432. doi: 10.1186/s12913-020-05273-8.
The Charlson Comorbidity Index (CCI) can be automatically calculated from the International Classification of Disease (ICD) code. However, the feasibility of this transformation has not been acknowledged, particularly in hospitals without a qualified ICD coding system. Here, we investigated the utility of coding-based CCI in China.
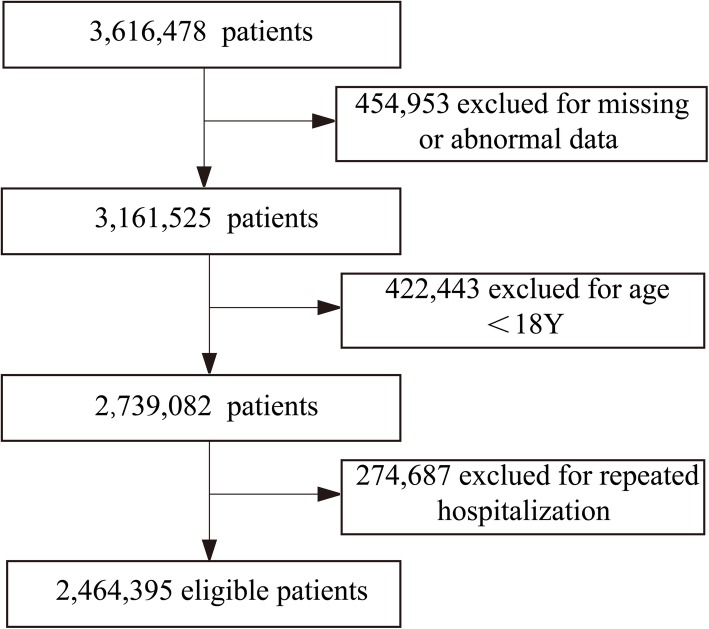
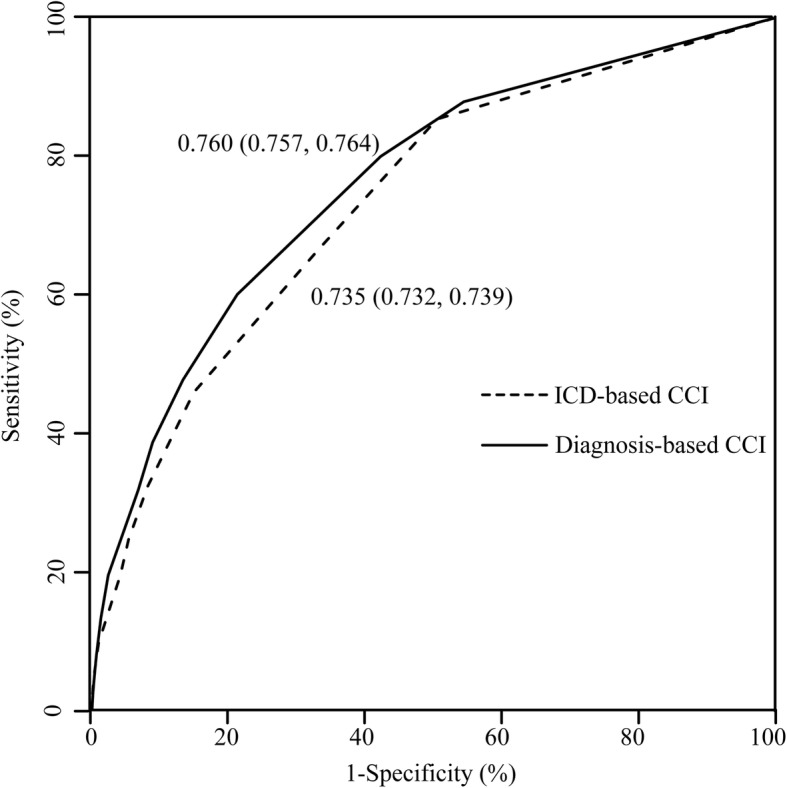
A multi-center, population-based, retrospective observational study was conducted, using a dataset incorporating 2,464,395 adult subjects from 15 hospitals. CCI was calculated using both ICD-10-based and diagnosis-based method, according to the transformation rule reported previously and to the literal description from discharge diagnosis, respectively. A κ coefficient of variation was used as a measure of agreement between the above two methods for each hospital. The discriminative abilities of the two methods were compared using the receiver-of-operating characteristic curve (ROC) for prediction of in-hospital mortality.
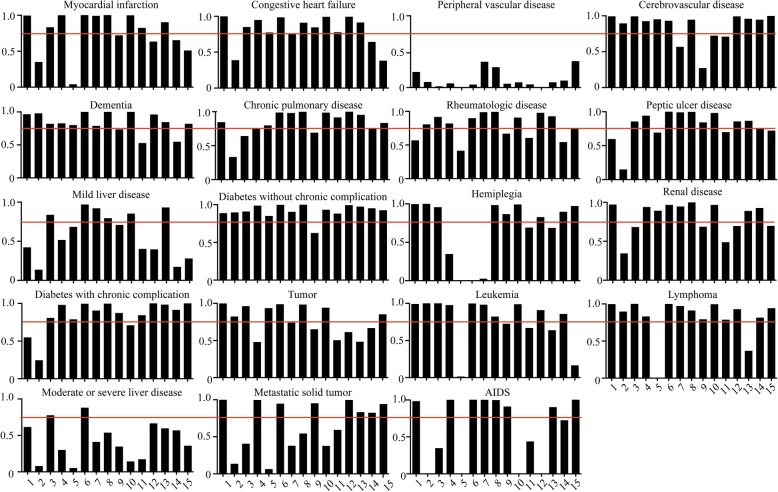
Total agreement between the ICD-based and diagnosis-based CCI for each index ranged from 86.1 to 100%, with κ coefficients from 0.210 [95% confidence interval (CI) 0.208-0.212] to 0.932 (95% CI 0.924-0.940). None of the 19 indices of CCI had a κ coefficient > 0.75 in all the hospitals included for study. The area under the curve of ROC for in-hospital mortality of all 15 hospitals was significantly lower for ICD-based than diagnosis-based CCI [0.735 (0.732, 0.739) vs 0.760 (0.757, 0.764)], indicative of more limited discriminative ability of the ICD-based calculation.
CCI calculated using ICD-10 coding did not agree with diagnosis-based CCI. ICD-based CCI displayed diminished discrimination performance in terms of in-hospital mortality, indicating that this method is not promising for CCI scoring in China under the present circumstances.
查尔森合并症指数(CCI)可根据国际疾病分类(ICD)编码自动计算得出。然而,这种转换的可行性尚未得到认可,尤其是在没有合格ICD编码系统的医院。在此,我们调查了基于编码的CCI在中国的实用性。
进行了一项多中心、基于人群的回顾性观察研究,使用了包含来自15家医院的2464395名成年受试者的数据集。分别根据先前报告的转换规则和出院诊断的文字描述,使用基于ICD - 10的方法和基于诊断的方法计算CCI。使用κ变异系数作为衡量每家医院上述两种方法之间一致性的指标。使用受试者操作特征曲线(ROC)比较两种方法对院内死亡率预测的判别能力。
基于ICD的CCI和基于诊断的CCI在各指标上的总体一致性范围为86.1%至100%,κ系数范围为0.210[95%置信区间(CI)0.208 - 0.212]至0.932(95%CI 0.924 - 0.940)。在纳入研究的所有医院中,CCI的19项指标中没有一项κ系数>0.75。所有15家医院基于ICD的CCI对院内死亡率的ROC曲线下面积显著低于基于诊断的CCI[0.735(0.732,0.739)对0.760(0.757,0.764)],表明基于ICD的计算判别能力更有限。
使用ICD - 10编码计算的CCI与基于诊断的CCI不一致。基于ICD的CCI在院内死亡率方面的判别性能下降,表明在当前情况下,该方法在中国用于CCI评分没有前景。