Strain W David, Tsang Carmen, Hurst Michael, McEwan Phil, Unadkat Minesh, Meadowcroft Simon, Shardlow Richard, Evans Marc
Diabetes and Vascular Research Centre, University of Exeter Medical School, Exeter, UK.
Health Economics and Outcomes Research Ltd., Cardiff, UK.
Diabetes Ther. 2020 Jun;11(6):1381-1395. doi: 10.1007/s13300-020-00834-w. Epub 2020 May 18.
Metformin is the recommended initial treatment in type 2 diabetes mellitus (T2DM), but when this does not give adequate glucose control the choice of which second-line drug to use is uncertain as none have been found to have a better overall glycaemic response. In this real-world study dipeptidyl peptidase 4 inhibitors (DPP4i), sulphonylureas (SU), thiazolidinediones (TZD) and sodium glucose co-transporter 2 inhibitors (SGLT2i) were compared for their effectiveness in lowering glycated haemoglobin (HbA1c) levels for a particular individual based on their clinical characteristics.
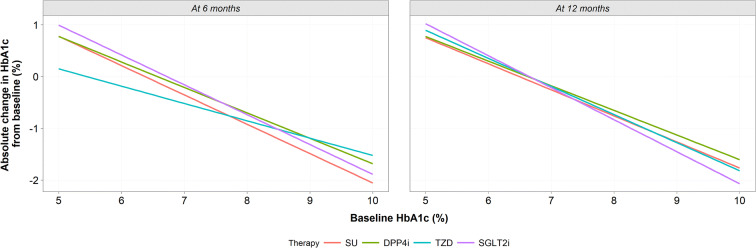
A retrospective analysis was undertaken of electronic health records of people with T2DM prescribed metformin alongside a DPP4i, SU, TZD or SGLT2i at second-line. Regression modelling was used to model the changes in HbA1c from baseline at month 6 and month 12 for the individual therapies, adjusting for demographic and clinical characteristics.
There were 7170 people included in the study. Treatment at second-line with SUs, DPP4i, TZDs and SGLT2i resulted in similar percentages of people achieving the recommended HbA1c target of < 7.5% (58 mmol/mol) at both 6 and 12 months. For those receiving SGLT2i and SUs, the greatest improvement in HbA1c was observed in relatively younger and older people, respectively. Trends were detected between other baseline characteristics and HbA1c improvement by drug class, but they were not statistically significant. Non-adherence rates were low for all drug classes. People with a higher medication possession ratio (≥ 80%) also had greater improvements in HbA1c at 12 months.
This study identified patients' phenotypic characteristics that may have the potential to influence individual treatment response. Accounting for these characteristics in clinical treatment decisions may facilitate individualised prescribing by being able to select the right drug for the right patient.
二甲双胍是2型糖尿病(T2DM)的推荐初始治疗药物,但当血糖控制不佳时,由于尚未发现哪种二线药物具有更好的总体血糖反应,因此选择使用哪种二线药物并不明确。在这项真实世界研究中,比较了二肽基肽酶4抑制剂(DPP4i)、磺脲类药物(SU)、噻唑烷二酮类药物(TZD)和钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i)根据特定个体的临床特征降低糖化血红蛋白(HbA1c)水平的有效性。
对接受二甲双胍治疗且二线使用DPP4i、SU、TZD或SGLT2i的T2DM患者的电子健康记录进行回顾性分析。采用回归模型对各治疗方案在第6个月和第12个月时HbA1c相对于基线的变化进行建模,并对人口统计学和临床特征进行调整。
该研究共纳入7170人。二线使用SU、DPP4i、TZD和SGLT2i治疗的患者在6个月和12个月时达到推荐的HbA1c目标(<7.5%,即58 mmol/mol)的比例相似。对于接受SGLT2i和SU治疗的患者,分别在相对年轻和年长的人群中观察到HbA1c的最大改善。在其他基线特征与不同药物类别导致的HbA1c改善之间检测到了趋势,但无统计学意义。所有药物类别的不依从率均较低。药物持有率较高(≥80%)的患者在12个月时HbA1c的改善也更大。
本研究确定了可能影响个体治疗反应的患者表型特征。在临床治疗决策中考虑这些特征,通过为合适的患者选择合适的药物,可能有助于个体化处方。