Innovation, Implementation and Clinical Translation in Health (IIMPACT), School of Health Sciences, University of South Australia, Adelaide, SA 5000, Australia.
Australian Centre of Precision Health, School of Health Sciences, University of South Australia, Adelaide, SA 5000, Australia.
Int J Chron Obstruct Pulmon Dis. 2020 Apr 23;15:903-919. doi: 10.2147/COPD.S178049. eCollection 2020.
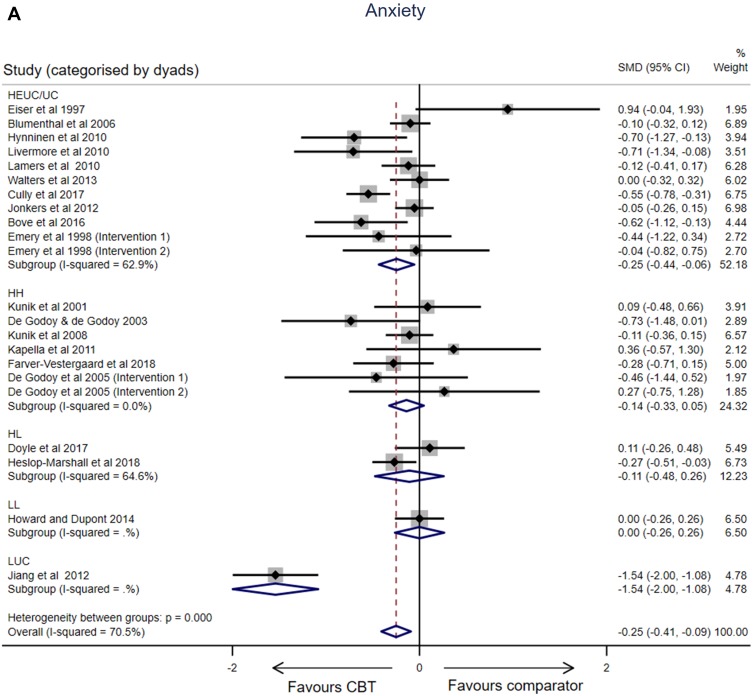
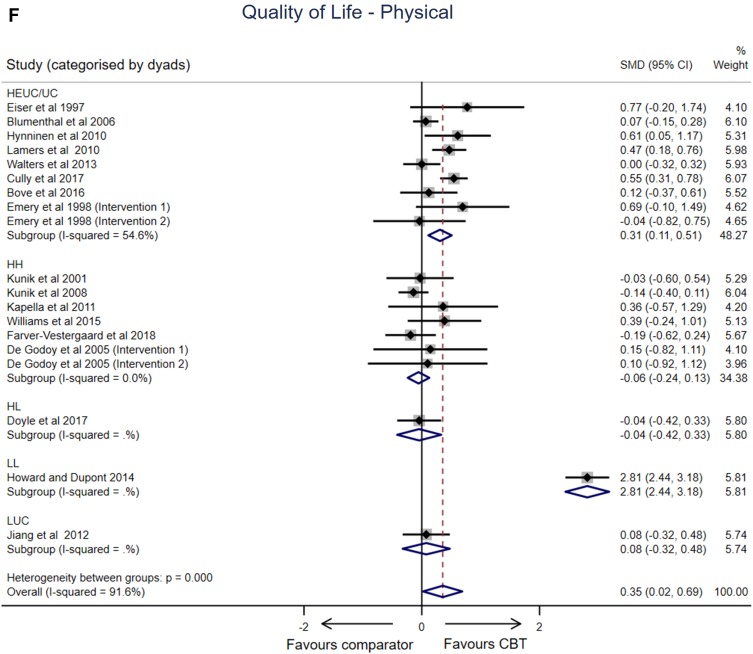
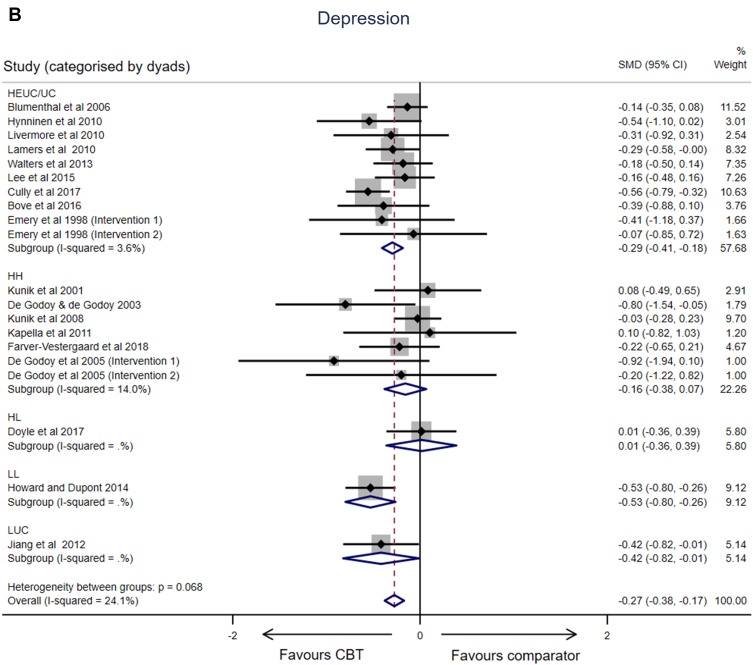
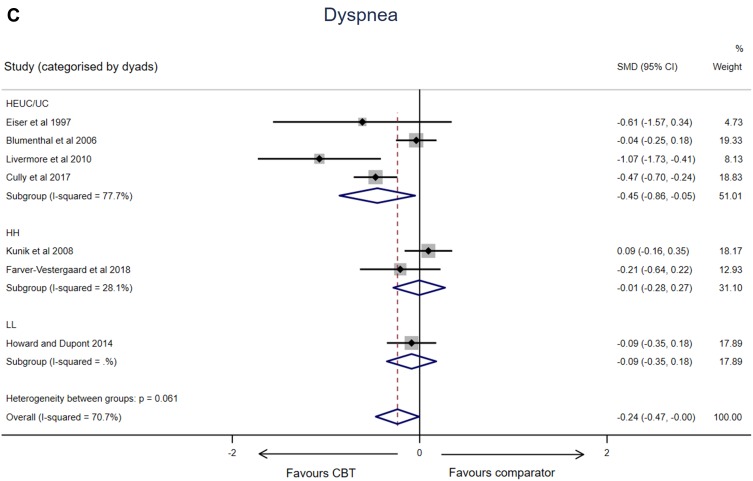
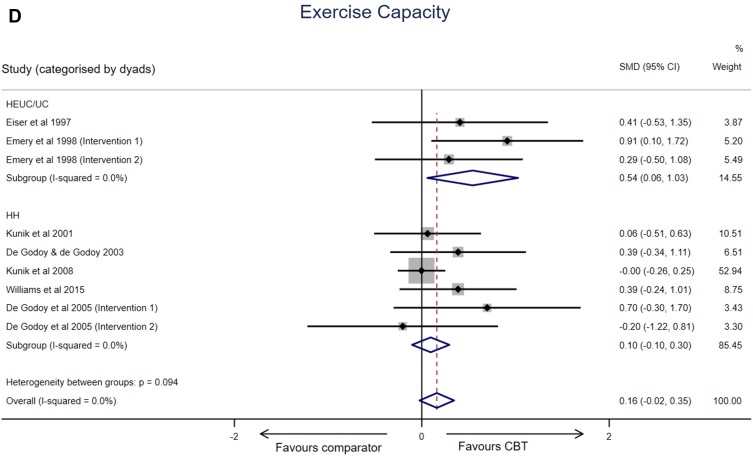
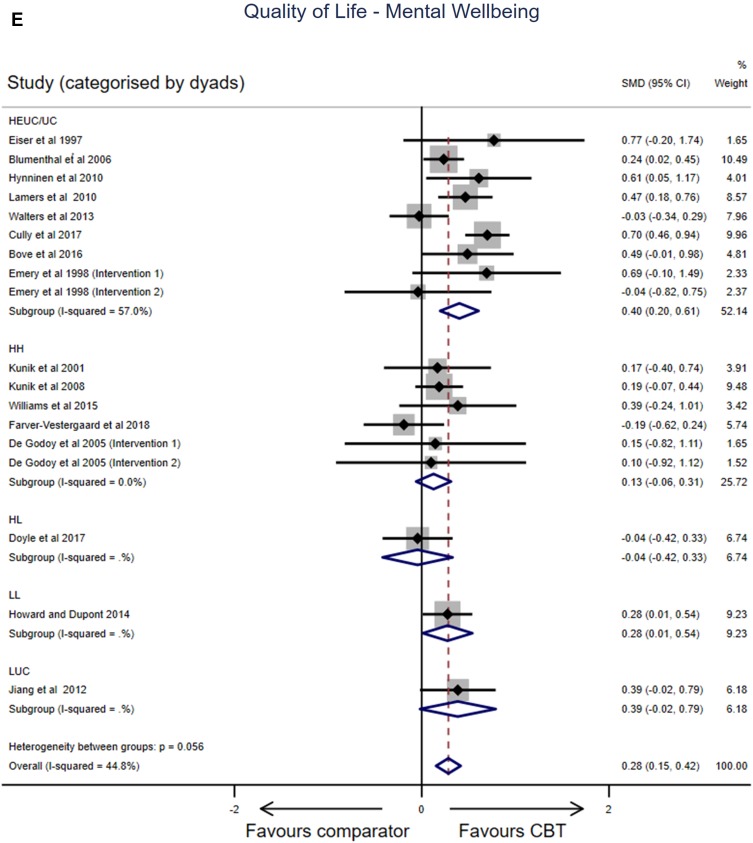
Cognitive behavioral therapy (CBT) is increasingly recommended in the management of people living with chronic obstructive pulmonary disease (COPD). This rapid review presents the evidence base for CBT for people with COPD and describes 1) the nature of CBT interventions and comparators in controlled trials (high or low resource intensity); and 2) factors influencing intervention effects on health outcomes (anxiety, depression, breathlessness, quality of life and exercise capacity). Primary studies reporting CBT interventions in adults with COPD were identified with data extracted by a single reviewer (20% of studies checked for data accuracy). Studies were synthesized descriptively with meta-analyses (random effects models) of controlled trials undertaken to report mean standardized effect sizes (95% CI) for health outcomes. Random effects meta-regression models explored whether CBT target, intervention dosage, intensity, facilitator profession, delivery mode, clinically significant anxiety/depression, trial design/quality and sample size predicted effect size. The search identified 33 primary studies published between 1996 and 2019 (controlled trials n=24, single group cohort n=6, case exemplars n=2, phenomenological n=1). Controlled trials frequently compared high-intensity CBT interventions against enhanced/usual care (n=12) or high-intensity CBT interventions against high-intensity comparators (n=11). When all controlled studies were included, small, significant improvements favoring CBT were evident across all health outcomes (SMD ranged from -0.27 to 0.35, p<0.05). When intensity dyads were considered, significant improvements were evident only when high-intensity CBT interventions were compared to enhanced usual care/usual care (SMDs ranged from -0.45 to 0.54, p <0.05). No other variable consistently predicted intervention effect sizes across all health outcomes. Overall, the evidence base supports the use of CBT for a range of health outcomes in people with COPD. Consistent benefits were evident when high-resource-intensive CBT interventions were compared to usual care. Low-resource-intensity CBT warrants further investigation in settings where cost of comprehensive care is prohibitive.
认知行为疗法(CBT)在慢性阻塞性肺疾病(COPD)患者的管理中越来越受到推荐。本快速综述介绍了 CBT 用于 COPD 患者的证据基础,并描述了 1)对照试验中 CBT 干预措施和对照措施的性质(高或低资源强度);2)影响干预对健康结果(焦虑、抑郁、呼吸困难、生活质量和运动能力)影响的因素。通过一名评审员(对 20%的研究进行数据准确性检查)单独提取数据,确定了报告 COPD 成人 CBT 干预措施的主要研究。对对照试验进行了描述性综合分析,以报告健康结果的标准化均数效应大小(95%CI)。随机效应荟萃回归模型探讨了 CBT 目标、干预剂量、强度、促进者专业、交付模式、临床显著焦虑/抑郁、试验设计/质量和样本量是否预测效应大小。检索确定了 1996 年至 2019 年期间发表的 33 项主要研究(对照试验 n=24,单组队列 n=6,病例实例 n=2,现象学 n=1)。对照试验经常将高强度 CBT 干预措施与增强/常规护理(n=12)或高强度 CBT 干预措施与高强度对照措施(n=11)进行比较。当纳入所有对照研究时,所有健康结果均显示出有利于 CBT 的小而显著的改善(SMD 范围为 -0.27 至 0.35,p<0.05)。当考虑强度对时,只有当高强度 CBT 干预措施与增强常规护理/常规护理相比时,才会出现显著改善(SMD 范围为 -0.45 至 0.54,p <0.05)。没有其他变量能够在所有健康结果中一致预测干预效果大小。总体而言,证据基础支持 CBT 用于 COPD 患者的一系列健康结果。当高强度资源密集型 CBT 干预措施与常规护理相比时,可观察到一致的益处。在综合护理成本过高的情况下,低资源密集型 CBT 值得进一步研究。