Vora Surabhi B, Waghmare Alpana, Englund Janet A, Qu Pingping, Gardner Rebecca A, Hill Joshua A
Department of Pediatrics, University of Washington, Seattle, Washington, USA.
Seattle Children's Research Institute, Seattle, Washington, USA.
Open Forum Infect Dis. 2020 Apr 9;7(5):ofaa121. doi: 10.1093/ofid/ofaa121. eCollection 2020 May.
Infectious complications of chimeric antigen receptor (CAR) T-cell immunotherapy in children and young adults have not been well described.
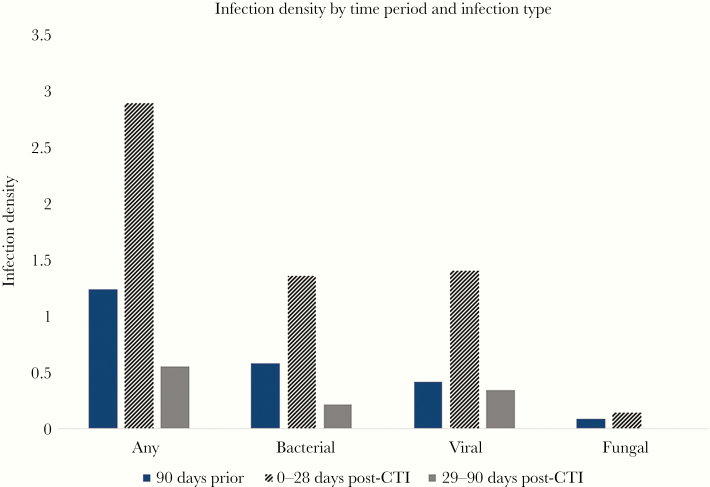
Medical records of patients ≤26 years old receiving CD19 CAR T-cell infusion (CTI) at a single institution between 2014 and 2017 were reviewed. The number of infections per 100 days-at-risk (infection density) in the 90 days preceding and 0-28 and 29-90 days after CTI was calculated. Poisson regression and Cox analyses were utilized to identify risk factors for infections.
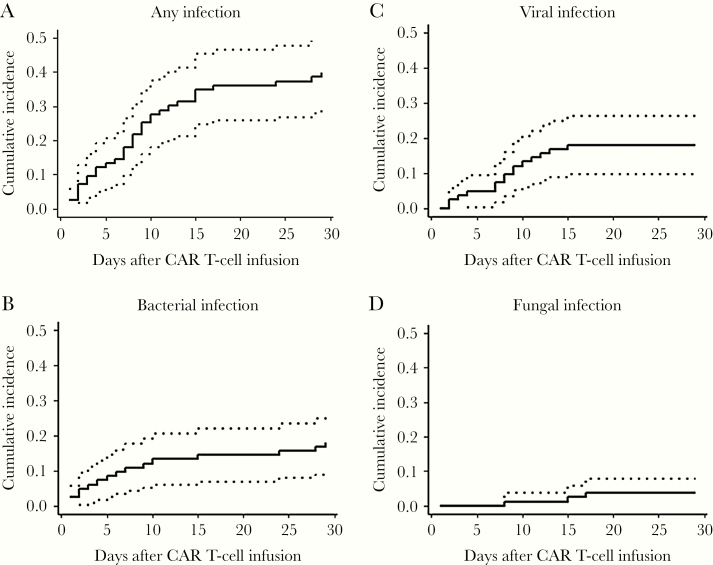
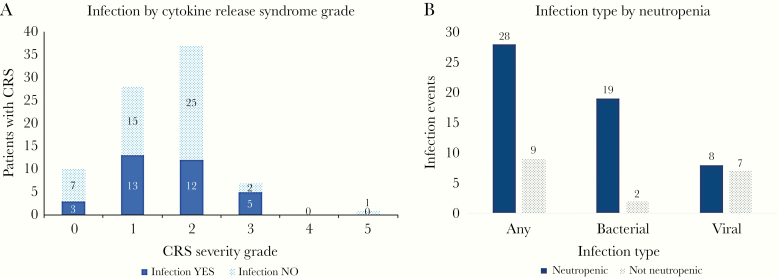
Eighty-three patients received CTI during the study period. Most patients (98%) had refractory or relapsed acute lymphoblastic leukemia (ALL). Infections occurred in 54% of patients in the 90 days before CTI (infection density, 1.23) and in 40% of patients in the first 28 days following CTI (infection density, 2.89). Infection density decreased to 0.55 in the 29-90 days post-CTI. Most infections were bacteremias (39%) or respiratory viral infections (43%). Pre-CTI risk factors associated with infection included prior hematopoietic cell transplantation (HCT), immunoglobulin G (IgG) level <400 mg/dL, and lymphodepletion other than cyclophosphamide plus fludarabine; post-CTI risk factors included higher-severity CRS and IgG <400 mg/dL.
Infection rates in children and young adults receiving CD19 CAR T-cell therapy increase in the first month and then decline. Understanding types and timing of infections and contributing risk factors may help inform prophylactic and monitoring strategies. Specific attention should be given to patients with prior HCT, severe hypogammaglobulinemia, and severe CRS.
嵌合抗原受体(CAR)T细胞免疫疗法在儿童和青年中的感染并发症尚未得到充分描述。
回顾了2014年至2017年间在单一机构接受CD19 CAR T细胞输注(CTI)的26岁及以下患者的病历。计算了CTI前90天、CTI后0 - 28天和29 - 90天每100天的感染数(感染密度)。采用泊松回归和Cox分析来确定感染的危险因素。
在研究期间,83例患者接受了CTI。大多数患者(98%)患有难治性或复发性急性淋巴细胞白血病(ALL)。CTI前90天,54%的患者发生感染(感染密度为1.23);CTI后前28天,40%的患者发生感染(感染密度为2.89)。CTI后29 - 90天,感染密度降至0.55。大多数感染为菌血症(39%)或呼吸道病毒感染(43%)。与感染相关的CTI前危险因素包括既往造血细胞移植(HCT)、免疫球蛋白G(IgG)水平<400 mg/dL以及除环磷酰胺加氟达拉滨之外的淋巴细胞清除;CTI后危险因素包括更高严重程度的细胞因子释放综合征(CRS)和IgG<400 mg/dL。
接受CD19 CAR T细胞治疗的儿童和青年的感染率在第一个月升高,然后下降。了解感染类型、时间及相关危险因素可能有助于制定预防和监测策略。应特别关注既往有HCT、严重低丙种球蛋白血症和严重CRS的患者。