Linder Jeffrey A, Weissman Joel S, Reyes Nieva Harry, Lipsitz Stuart, Haring R Sterling, DeAngelis Julie, Kristy Rita M, Loughlin Kevin R
Division of General Internal Medicine and Geriatrics, Northwestern University Feinberg School of Medicine, 750 N. Lake Shore Drive, 10th Floor, Chicago, IL, 60611, USA.
Center for Surgery and Public Health, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
BMC Health Serv Res. 2020 May 20;20(1):447. doi: 10.1186/s12913-020-05315-1.
Overactive bladder (OAB) is common and morbid. Medication and diagnosis claims may be specific, but lack sensitivity to identify patients with overactive bladder. We used an "electronic health record (EHR) phenotype" to identify cases and describe treatment choices and anticholinergic burden for OAB.
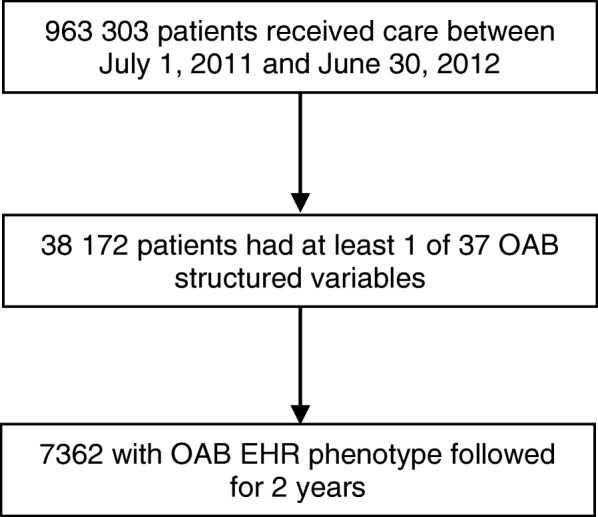
We conducted a retrospective cohort study in a large, integrated health delivery system between July 2011 and June 2012 (2-year follow-up). We examined care from primary care and specialty clinics, medication and procedure use, and anticholinergic burden for each patient.
There were 7362 patients with an EHR OAB phenotype; 50% of patients were > 65 years old, 74% were female, and 83% were white. The distribution of care included primary care physician (PCP)/specialty co-management (25% of patients); PCP care only (18%); urology only (13%); or some other combination of specialty care (33%). Only 40% of patients were prescribed at least 1 OAB medication during the study. The mean duration of prescribed medication was 1.5 months (95% confidence interval [CI], 1.4 to 1.6 months; range, < 1 month to 24 months). Independent predictors of receipt of an OAB medication included increasing age (odds ratio [OR], 1.4 for every 10 years; 95% CI, 1.4 to 1.5), women (OR, 1.6 compared with men; 95% CI, 1.4 to 1.8), diabetes (OR, 1.3; 95% CI, 1.1 to 1.5), and certain sources of care compared with PCP-only care: PCP/specialty co-management (OR, 1.8; 95% CI, 1.5 to 2.0), urology (OR, 2.2; 95% CI, 1.8 to 2.6), and multiple specialists (OR, 1.4; 95% CI, 1.2 to 1.8). Very few patients received other treatments: biofeedback (< 1%), onabotulinumtoxinA (2%), or sacral nerve stimulation (1%). Patients who received OAB medications had significantly higher anticholinergic burden than patients who did not (anticholinergic total standardized daily dose, 125 versus 46; P < .001).
Although OAB is common and morbid, in a longitudinal study using an EHR OAB phenotype 40% of patients were treated with OAB medication and only briefly.
膀胱过度活动症(OAB)常见且具有危害性。药物治疗和诊断声明可能具有特异性,但在识别膀胱过度活动症患者方面缺乏敏感性。我们使用“电子健康记录(EHR)表型”来识别病例,并描述膀胱过度活动症的治疗选择和抗胆碱能负担。
我们在2011年7月至2012年6月期间(2年随访),在一个大型综合医疗服务系统中进行了一项回顾性队列研究。我们检查了每位患者从初级保健和专科诊所获得的护理、药物和手术使用情况以及抗胆碱能负担。
有7362例具有EHR膀胱过度活动症表型的患者;50%的患者年龄大于65岁,74%为女性,83%为白人。护理分布包括初级保健医生(PCP)/专科联合管理(25%的患者);仅PCP护理(18%);仅泌尿外科护理(13%);或专科护理的其他某种组合(33%)。在研究期间,只有40%的患者至少开具了1种膀胱过度活动症药物。开具药物的平均持续时间为1.5个月(95%置信区间[CI],1.4至1.6个月;范围,<1个月至24个月)。接受膀胱过度活动症药物治疗的独立预测因素包括年龄增长(每10年优势比[OR]为1.4;95%CI,1.4至1.5)、女性(与男性相比OR为1.6;95%CI,1.4至1.8)、糖尿病(OR为1.3;95%CI,1.1至1.5),以及与仅接受PCP护理相比的某些护理来源:PCP/专科联合管理(OR为1.8;95%CI,1.5至2.0)、泌尿外科(OR为2.2;95%CI,1.8至2.6)和多个专科医生(OR为1.4;95%CI,1.2至1.8)。很少有患者接受其他治疗:生物反馈(<1%)、A型肉毒毒素(2%)或骶神经刺激(1%)。接受膀胱过度活动症药物治疗的患者的抗胆碱能负担明显高于未接受治疗的患者(抗胆碱能总标准化日剂量,125对46;P<0.001)。
尽管膀胱过度活动症常见且具有危害性,但在一项使用EHR膀胱过度活动症表型的纵向研究中,40%的患者接受了膀胱过度活动症药物治疗,且治疗时间短暂。