Pati Manoj Kumar, Swaroop N, Kar Arin, Aggarwal Preeti, Jayanna Krishnamurthy, Van Damme Wim
1Karnataka Health Promotion Trust, IT Park, 5th floor, 1-4, Rajajinagar Industrial Area behind KSSIDC Admin Office, Rajajinagar, Bangalore, Karnataka 560044 India.
Social Initiatives, Landmark Group, Bangalore, India.
Public Health Rev. 2020 May 13;41:8. doi: 10.1186/s40985-020-00128-3. eCollection 2020.
Low- and middle-income countries (LMICs) account for a higher burden of noncommunicable diseases (NCD) and home to a higher number of premature deaths (before age 70) from NCDs. NCDs have become an integral part of the global development agenda; hence, the scope of action on NCDs extends beyond just the health-related sustainable development goal (SDG 3). However, the organization and integration of NCD-related health services have faced several gaps in the LMIC regions such as India. Although the national NCD programme of India has been in operation for a decade, challenges remain in the integration of NCD services at primary care. In this paper, we have analysed existing gaps in the organization and integration of NCD services at primary care and suggested plausible solutions that exist.
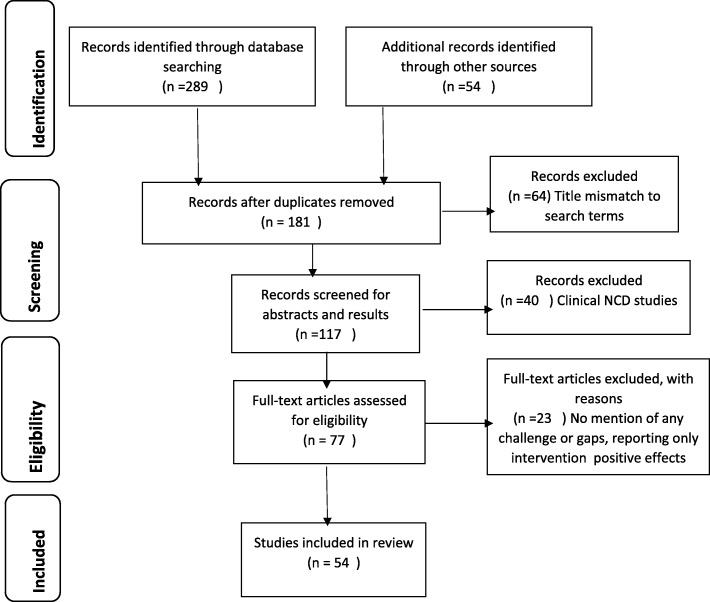
The identification of gaps is based out of a review of peer-reviewed articles, reports on national and global guidelines/protocols. The gaps are organized and narrated at four levels such as community, facility, health system, health policy and research, as per the WHO Innovative Care for Chronic Conditions framework (WHO ICCC).
The review found that challenges in the identification of eligible beneficiaries, shortage and poor capacity of frontline health workers, poor functioning of community groups and poor community knowledge on NCD risk factors were key gaps at the community level. Challenges at facility level such as poor facility infrastructure, lack of provider knowledge on standards of NCD care and below par quality of care led to poor management of NCDs. At the health system level, we found, organization of care, programme management and monitoring systems were not geared up to address NCDs. Multi-sectoral collaboration and coordination were proposed at the policy level to tackle NCDs; however, gaps remained in implementation of such policies. Limited research on the effect of health promotion, prevention and, in particular, non-medical interventions on NCDs was found as a key gap at the research level.
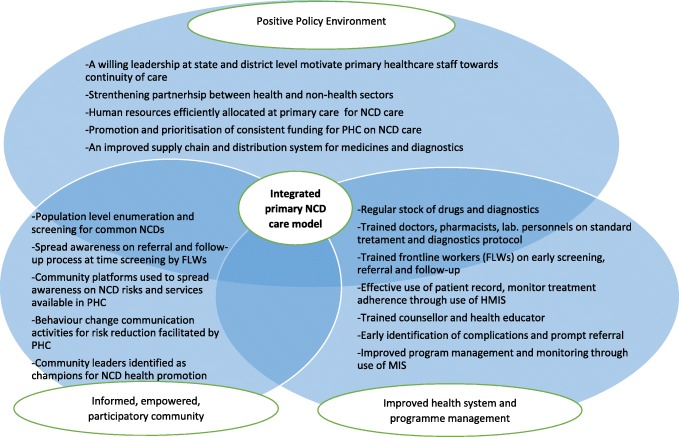
This paper reinforces the need for an integrated comprehensive model of NCD care especially at primary health care level to address the growing burden of these diseases. This overarching review is quite relevant and useful in organizing NCD care in Indian and similar LMIC settings.
低收入和中等收入国家(LMICs)的非传染性疾病(NCD)负担较重,且70岁之前死于非传染性疾病的过早死亡人数较多。非传染性疾病已成为全球发展议程的一个组成部分;因此,非传染性疾病的行动范围不仅限于与健康相关的可持续发展目标(SDG 3)。然而,在印度等LMIC地区,与非传染性疾病相关的卫生服务的组织和整合面临着一些差距。尽管印度的国家非传染性疾病计划已经实施了十年,但在初级保健中整合非传染性疾病服务方面仍然存在挑战。在本文中,我们分析了初级保健中非传染性疾病服务的组织和整合方面存在的现有差距,并提出了可行的解决方案。
通过对同行评审文章、国家和全球指南/协议报告的回顾来确定差距。根据世界卫生组织慢性病创新照护框架(WHO ICCC),这些差距在社区、机构、卫生系统、卫生政策和研究四个层面进行组织和阐述。
审查发现,在社区层面,确定合格受益人的挑战、一线卫生工作者短缺和能力不足、社区团体运作不佳以及社区对非传染性疾病危险因素的认识不足是关键差距。机构层面的挑战,如机构基础设施差、提供者对非传染性疾病护理标准的知识缺乏以及护理质量低于标准,导致了非传染性疾病的管理不善。在卫生系统层面,我们发现,护理组织、项目管理和监测系统没有做好应对非传染性疾病的准备。在政策层面,提出了多部门合作与协调以应对非传染性疾病;然而,这些政策的实施仍存在差距。在研究层面,发现对健康促进、预防,特别是非医疗干预对非传染性疾病影响的研究有限是一个关键差距。
本文强调了建立非传染性疾病综合护理模式的必要性,特别是在初级卫生保健层面,以应对这些疾病日益加重的负担。这一全面审查对于在印度和类似的LMIC环境中组织非传染性疾病护理非常相关且有用。