Bronner Murrison Liza, Ananthakrishnan Ramya, Sukumar Sumanya, Augustine Sheela, Krishnan Nalini, Pai Madhukar, Dowdy David W
Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America.
Center for Tuberculosis Research, Johns Hopkins University, Baltimore, Maryland, United States of America.
PLoS One. 2016 Feb 22;11(2):e0149862. doi: 10.1371/journal.pone.0149862. eCollection 2016.
Private practitioners are frequently the first point of healthcare contact for patients with tuberculosis (TB) in India. Inappropriate TB management practices among private practitioners may contribute to delayed TB diagnosis and generate drug resistance. However, these practices are not well understood. We evaluated diagnostic and treatment practices for active TB and benchmarked practices against International Standards for TB Care (ISTC) among private medical practitioners in Chennai.
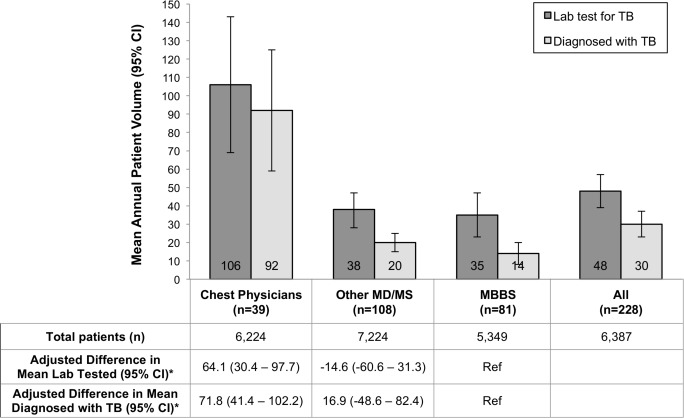
A cross-sectional survey of 228 practitioners practicing in the private sector from January 2014 to February 2015 in Chennai city who saw at least one TB patient in the previous year. Practitioners were randomly selected from both the general community and a list of practitioners who referred patients to a public-private mix program for TB treatment in Chennai. Practitioners were interviewed using standardized questionnaires.
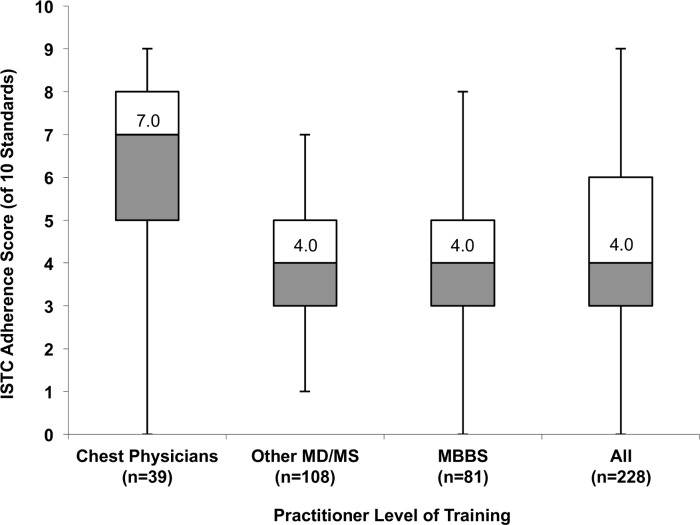
Among 228 private practitioners, a median of 12 (IQR 4-28) patients with TB were seen per year. Of 10 ISTC standards evaluated, the median of standards adhered to was 4.0 (IQR 3.0-6.0). Chest physicians reported greater median ISTC adherence than other MD and MS practitioners (score 7.0 vs. 4.0, P<0.001), or MBBS practitioners (score 7.0 vs. 4.0, P<0.001). Only 52% of all practitioners sent >5% of patients with cough for TB testing, 83% used smear microscopy for diagnosis, 33% monitored treatment response, and 22% notified TB cases to authorities. Of 228 practitioners, 68 reported referring all patients with new pulmonary TB for treatment, while 160 listed 27 different regimens; 78% (125/160) prescribed a regimen classified as consistent with ISTC. Appropriate treatment practices differed significantly between chest physicians and other MD and MS practitioners (54% vs. 87%, P<0.001).
TB management practices in India's urban private sector are heterogeneous and often suboptimal. Private providers must be better engaged to improve diagnostic capacity and decrease TB transmission in the community.
在印度,私人执业医生通常是结核病患者就医的首要接触点。私人执业医生中不恰当的结核病管理做法可能导致结核病诊断延迟并产生耐药性。然而,这些做法并未得到充分了解。我们评估了钦奈私人执业医生对活动性结核病的诊断和治疗做法,并将这些做法与《国际结核病防治标准》(ISTC)进行了对比。
对2014年1月至2015年2月在钦奈市私营部门执业且上一年至少诊治过1例结核病患者的228名医生进行横断面调查。医生从普通社区以及将患者转诊至钦奈公私混合结核病治疗项目的医生名单中随机选取。使用标准化问卷对医生进行访谈。
在228名私人执业医生中,每年诊治的结核病患者中位数为12例(四分位间距4 - 28例)。在评估的10项ISTC标准中,遵循的标准中位数为4.0(四分位间距3.0 - 6.0)。胸部科医生报告的ISTC遵循程度中位数高于其他医学博士和医学硕士医生(得分7.0对4.0,P<0.001),也高于医学学士医生(得分7.0对4.0,P<0.001)。所有医生中只有52%将超过5%的咳嗽患者送去进行结核病检测,83%使用涂片显微镜检查进行诊断,33%监测治疗反应,22%向当局通报结核病病例。在228名医生中,68名报告将所有新发肺结核患者转诊进行治疗,而160名列出了27种不同的治疗方案;78%(125/160)开出的治疗方案被归类为符合ISTC。胸部科医生与其他医学博士和医学硕士医生的恰当治疗做法存在显著差异(54%对87%,P<0.001)。
印度城市私营部门的结核病管理做法参差不齐,且往往不够理想。必须更好地促使私人医疗服务提供者提高诊断能力并减少社区内的结核病传播。