Division of Pulmonary and Allergy, Department of Internal Medicine, College of Medicine, Yeungnam University and Regional Center for Respiratory Diseases, Yeungnam University Medical Center, Daegu, South Korea.
Division of Gastroenterology, Department of Internal Medicine, Yeungnam University Medical Center, College of Medicine, Yeungnam University, Daegu, South Korea.
Int J Chron Obstruct Pulmon Dis. 2020 May 7;15:1005-1014. doi: 10.2147/COPD.S249534. eCollection 2020.
Nonalcoholic fatty liver disease (NAFLD) is highly prevalent in patients with chronic obstructive pulmonary disease (COPD) and is independently associated with cardiometabolic comorbidities and systemic inflammation. Although several factors are associated with NAFLD, the influence of sarcopenia on NAFLD has not been fully determined in patients with COPD. We explored whether sarcopenia is associated with NAFLD in a COPD population.
Data from the Korean National Health and Nutrition Examination Surveys 2008-2011 were analyzed. The subjects were defined as having NAFLD when they had a hepatic steatosis index (HSI) score >36, which is a previously validated NAFLD prediction score. Sarcopenia_BMI (=total appendicular skeletal muscle mass [kg]/body mass index [kg/m]), sarcopenia_BW (=total appendicular skeletal muscle mass [kg]/body weight [kg] × 100), and sarcopenia_height (= total appendicular skeletal muscle mass (kg)/height (m)) measured using dual-energy X-ray absorptiometry was used to diagnose sarcopenia.
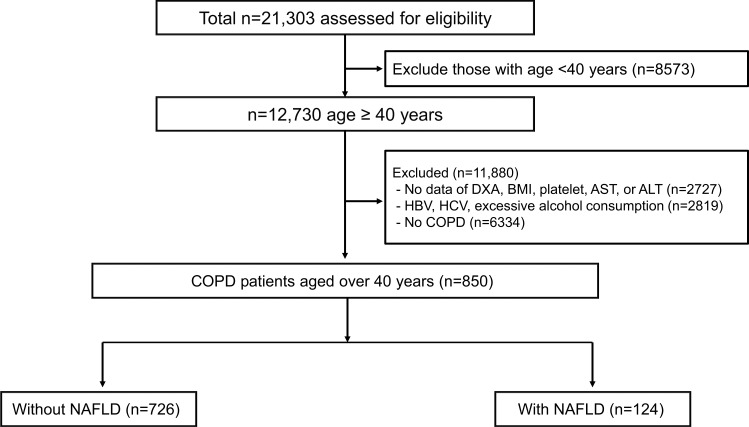
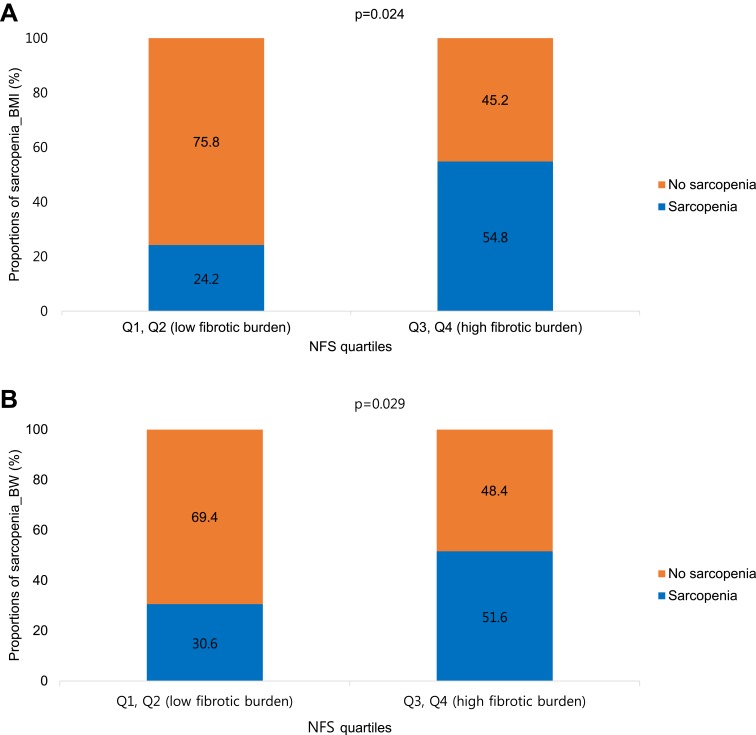
NAFLD was identified in 124 (14.6%) of 850 COPD subjects using the HSI. Multivariable logistic analyses adjusted for age, sex, hypertension, diabetes mellitus (DM), forced vital capacity (FVC), and metabolic syndrome demonstrated that sarcopenia (sarcopenia_BMI, odds ratio [OR] = 1.95; 95% confidence interval [CI], 1.11-3.46, p = 0.022; sarcopenia_BW, OR = 2.25; 95% CI, 1.30-3.92, p = 0.004) was associated with NAFLD in patients with COPD. The proportion of sarcopenia_BMI was higher in patients with a high fibrotic burden from NAFLD (Q3, Q4) than in subjects with a low fibrotic burden from NALFD (Q1, Q2) (54.8% vs 24.2%, p = 0.024). The proportion of sarcopenia_BW was also higher in patients with a high fibrotic burden from NAFLD than in patients with a low fibrotic burden from NAFLD (51.6% vs 30.6%, p = 0.029).
Sarcopenia was associated with an increased risk for NAFLD in patients with COPD, independent of age, sex, lung function, and metabolic factors. Sarcopenic COPD was also associated with a high fibrotic burden in NAFLD patients. Pulmonologists should be aware of possible liver comorbidities in the sarcopenic COPD phenotype.
非酒精性脂肪性肝病(NAFLD)在慢性阻塞性肺疾病(COPD)患者中患病率很高,并且与心脏代谢合并症和全身炎症独立相关。尽管有多种因素与 NAFLD 相关,但 COPD 患者中肌肉减少症对 NAFLD 的影响尚未完全确定。我们探讨了在 COPD 人群中肌肉减少症是否与 NAFLD 相关。
分析了 2008-2011 年韩国国家健康和营养检查调查的数据。当 HSI 评分>36 时,受试者被定义为患有 NAFLD,HSI 是先前验证的 NAFLD 预测评分。使用双能 X 射线吸收法测量的肌肉减少症-BMI(=全身骨骼肌质量[kg]/体重指数[kg/m])、肌肉减少症-BW(=全身骨骼肌质量[kg]/体重[kg]×100)和肌肉减少症-height(=全身骨骼肌质量[kg]/身高[m])用于诊断肌肉减少症。
使用 HSI 在 850 名 COPD 患者中发现了 124 名(14.6%)NAFLD 患者。多变量逻辑分析调整了年龄、性别、高血压、糖尿病(DM)、用力肺活量(FVC)和代谢综合征,结果表明肌肉减少症(肌肉减少症-BMI,比值比[OR] = 1.95;95%置信区间[CI],1.11-3.46,p = 0.022;肌肉减少症-BW,OR = 2.25;95%CI,1.30-3.92,p = 0.004)与 COPD 患者的 NAFLD 相关。NAFLD 纤维化负担较高(Q3、Q4)的患者中肌肉减少症-BMI 的比例高于 NAFLD 纤维化负担较低(Q1、Q2)的患者(54.8% vs 24.2%,p = 0.024)。NAFLD 纤维化负担较高的患者中肌肉减少症-BW 的比例也高于纤维化负担较低的患者(51.6% vs 30.6%,p = 0.029)。
肌肉减少症与 COPD 患者的 NAFLD 风险增加相关,与年龄、性别、肺功能和代谢因素无关。肌肉减少症合并 COPD 也与 NAFLD 患者的高纤维化负担相关。肺科医生应该意识到肌肉减少症合并 COPD 表型可能存在肝脏合并症。