Clinic for General and Interventional Cardiology/Angiology, Herz- und Diabeteszentrum NRW, Ruhr-Universität Bochum, Bad Oeynhausen, Germany.
Epidemiology and International Public Health, Bielefeld School of Public Health and Statistical Consulting Centre, Bielefeld University, Bielefeld, Germany.
Int J Cardiovasc Imaging. 2020 Oct;36(10):1821-1829. doi: 10.1007/s10554-020-01889-3. Epub 2020 May 22.
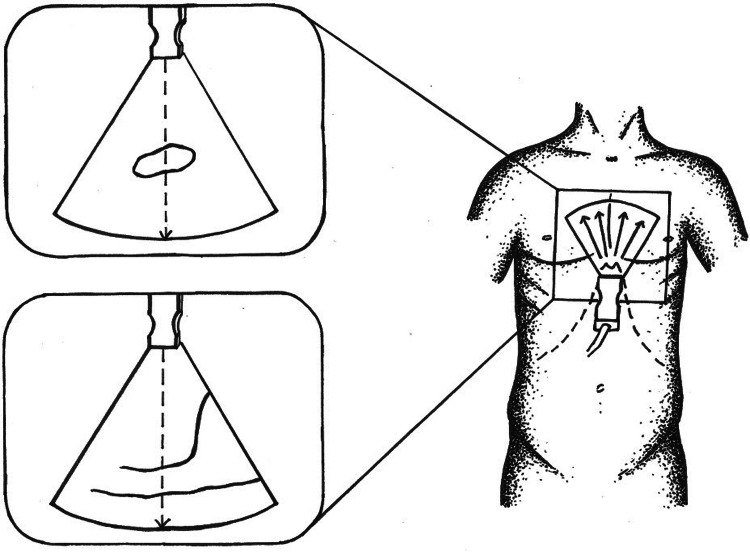
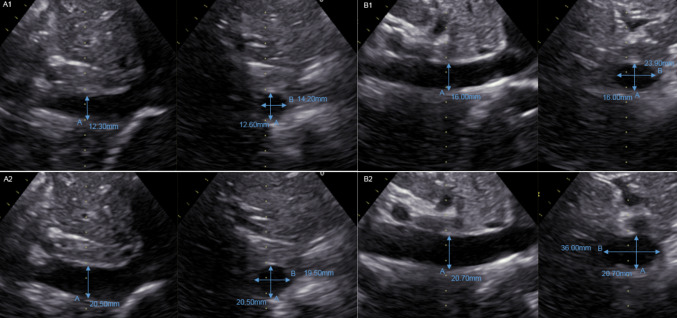
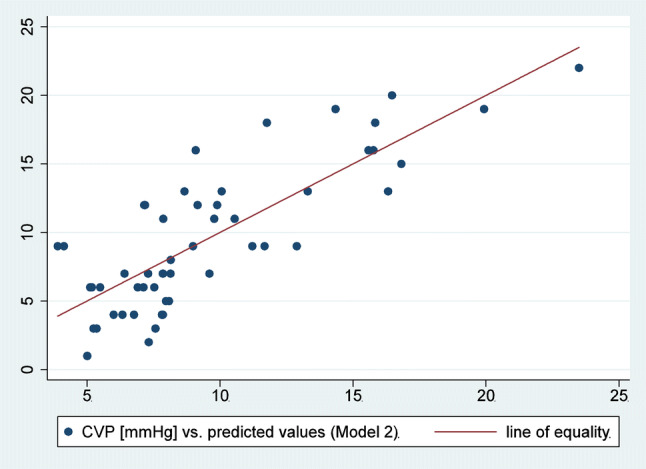
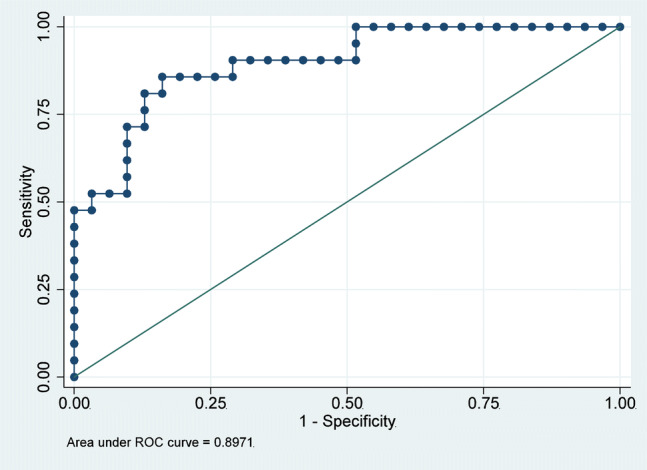
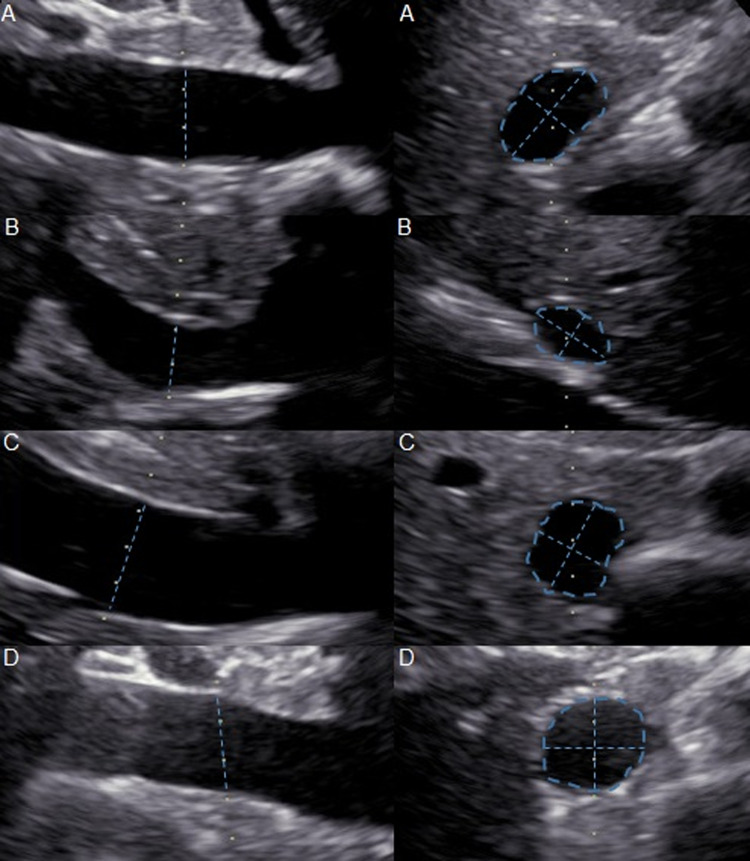
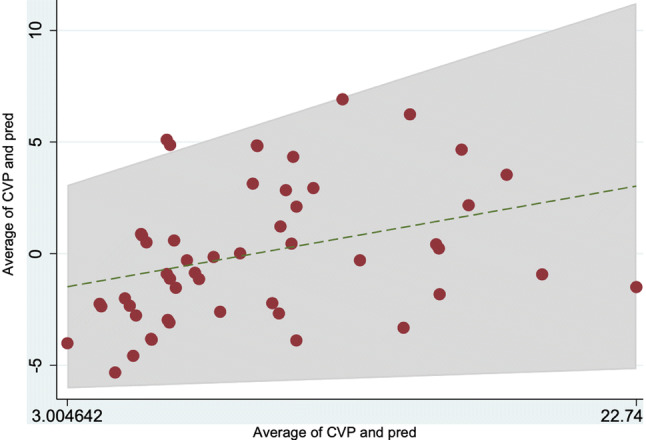
Assessing hemodynamics, especially central venous pressure (CVP), is essential in heart failure (HF). Right heart catheterization (RHC) is the gold-standard, but non-invasive methods are also needed. However, the role of 2-dimensional echocardiography (2DE) remains uncertain, and 3-dimensional echocardiography (3DE) is not always available. This study investigated standardized and breathing-corrected assessment of inferior vena cava (IVC) volume using echocardiography (2DE and 3DE) versus CVP determined invasively using RHC. Sixty consecutive HF patients were included (82% male, age 54 ± 11 years, New York Heart Association class 2.23 ± 0.8, ejection fraction 46 ± 18.4%, brain natriuretic peptide 696.93 ± 773.53 pg/mL). All patients underwent Swan-Ganz RHC followed by 2DE and 3DE, and IVC volume assessment. On 2DE, mean IVC size was 18.3 ± 5.5 mm and 13.8 ± 6 mm in the largest deflection and shortest distention, respectively. Mean CVP from RHC was 9.3 ± 5.3 mmHg. Neither 2DE nor 3DE showed acceptable correlation with invasively measured CVP; IVC volume acquisition showed optimal correlation with RHC CVP (0.64; 95% confidence interval 0.46-0.77), with better correlation when mitral valve early diastole E wave and right ventricular end-diastolic diameter were added. Using a CVP cut-point of 10 mmHg, receiver operating characteristic curve showed true positivity (specificity) of 0.90 and sensitivity of 62% for predicting CVP. A validation study confirmed these findings and verified the high predictive value of IVC volume assessment. Neither 2DE nor 3DE alone can reliably mirror CVP, but IVC volume acquisition using echocardiography allows non-invasive and adequate approximation of CVP. Correlation with invasively measured pressure was strongest when CVP is > 10 mmHg.
评估血流动力学,尤其是中心静脉压(CVP),在心衰(HF)中至关重要。右心导管检查(RHC)是金标准,但也需要非侵入性方法。然而,二维超声心动图(2DE)的作用仍不确定,且 3 维超声心动图(3DE)并非总是可用。本研究通过 RHC 确定的有创性测量 CVP 与超声心动图(2DE 和 3DE)评估下腔静脉(IVC)容量的标准化和呼吸校正评估进行比较,以研究该方法在 HF 患者中的应用。共纳入 60 例连续 HF 患者(82%为男性,年龄 54±11 岁,纽约心脏协会(NYHA)心功能分级 2.23±0.8,射血分数 46±18.4%,脑利钠肽 696.93±773.53 pg/mL)。所有患者均接受 Swan-Ganz RHC 检查,随后进行 2DE 和 3DE 检查,并进行 IVC 容量评估。2DE 下 IVC 平均大小为 18.3±5.5mm,最大变细和最短扩张时分别为 13.8±6mm。RHC 测量的平均 CVP 为 9.3±5.3mmHg。2DE 和 3DE 均与有创性测量的 CVP 无良好相关性;IVC 容量采集与 RHC CVP 相关性最佳(0.64;95%置信区间 0.46-0.77),当加入二尖瓣舒张早期 E 波和右心室舒张末期直径时相关性更好。当 CVP 截断值为 10mmHg 时,受试者工作特征曲线显示出预测 CVP 的真阳性(特异性)为 0.90,敏感性为 62%。验证研究证实了这些发现,并验证了 IVC 容量评估的高预测价值。2DE 和 3DE 均不能可靠地反映 CVP,但超声心动图采集的 IVC 容量可以进行非侵入性且充分地评估 CVP。当 CVP>10mmHg 时,与有创性测量压力的相关性最强。