Gyoten Takayuki, Schenk Sören, Rochor Kristin, Herwig Volker, Harnath Axel, Grimmig Oliver, Just Sören, Fritzsche Dirk, Messroghli Daniel
Department of Cardiovascular Surgery, Sana-Herzzentrum Cottbus, Leipziger Strasse 50, 03048, Cottbus, Germany.
Department of Cardiology, Sana-Herzzentrum Cottbus, Leipziger Strasse 50, 03048, Cottbus, Germany.
ESC Heart Fail. 2020 Aug;7(4):1781-1790. doi: 10.1002/ehf2.12741. Epub 2020 May 23.
The aim of this study was to compare the outcomes of surgical mitral valve repair or replacement (sMVR) and percutaneous edge-to-edge repair using MitraClip (pMVR) in patients with severe left ventricular dysfunction affected by functional mitral regurgitation (FMR).
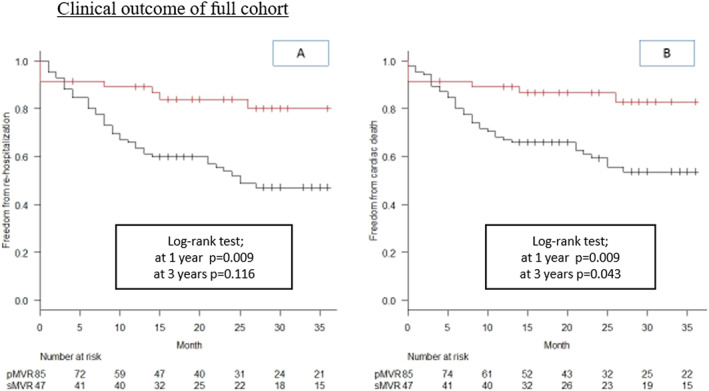
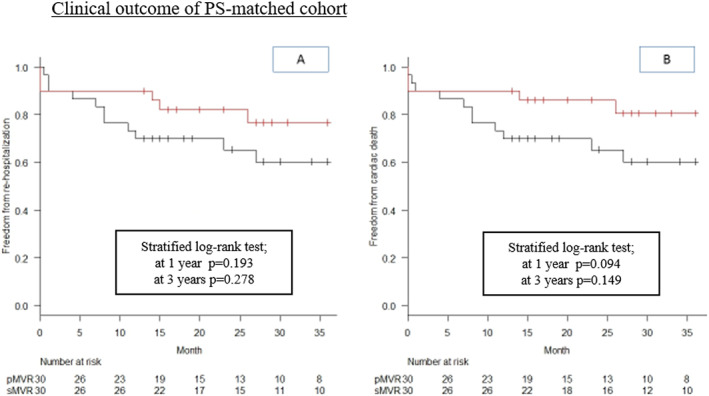
We retrospectively identified 132 patients with left ventricular ejection fraction (LVEF) ≦ 30% submitted to sMVR (n = 47) or pMVR (n = 85) for FMR at our centre from January 2013 to December 2017. To adjust for baseline imbalances, we used a propensity score matching by age, logistic EuroSCORE, and left ventricular end-systolic volume. After being matched, MitraClip therapy showed lower perioperative mortality and rate of complications yet increased residual mitral regurgitation (MR) grade than did surgery (0.2 ± 0.50 in sMVR vs. 1.3 ± 0.88 in pMVR, P < 0.0001). According to stratified multivariate Cox model analysis, residual MR severity was an independent risk factor for cardiac death [hazard ratio (HR), 2.81; 95% confidence interval [CI], 1.44-5.48, P = 0.0025] and re-hospitalization for heart failure (HR, 3.07; 95% CI, 1.50-6.29, P = 0.0022) at 1 year follow-up. Stratified multivariable Cox regression analysis at 3 years identified pMVR as risk factor for cardiac death (HR, 0.19; 95% CI, 0.040-0.86, P = 0.031) and re-hospitalization for heart failure (HR, 0.28; 95% CI, 0.077-0.99, P = 0.048).
In patients with FMR and LVEF ≤ 30%, MitraClip therapy resulted in lower perioperative complications and mortality than sMVR. However, surgically treated patients who survived the perioperative stage had less residual MR and experienced lower rates of re-hospitalization for heart failure at 1 year and lower cardiac mortality at 1 and 3 years of follow-up than did patients undergoing pMVR.
本研究旨在比较在因功能性二尖瓣反流(FMR)而出现严重左心室功能障碍的患者中,外科二尖瓣修复或置换术(sMVR)与使用MitraClip进行经皮缘对缘修复术(pMVR)的疗效。
我们回顾性纳入了2013年1月至2017年12月期间在本中心因FMR接受sMVR(n = 47)或pMVR(n = 85)治疗的132例左心室射血分数(LVEF)≤30%的患者。为了调整基线不平衡,我们采用倾向评分匹配法,匹配因素包括年龄、逻辑欧洲心脏手术风险评估系统(EuroSCORE)和左心室收缩末期容积。匹配后,MitraClip治疗组的围手术期死亡率和并发症发生率较低,但二尖瓣反流(MR)残余分级高于手术组(sMVR组为0.2±0.50,pMVR组为1.3±0.88,P<0.0001)。根据分层多变量Cox模型分析,在1年随访时,MR残余严重程度是心脏死亡[风险比(HR),2.81;95%置信区间(CI),1.44 - 5.48,P = 0.0025]和因心力衰竭再次住院(HR,3.07;95%CI,1.50 - 6.29,P = 0.0022)的独立危险因素。3年时的分层多变量Cox回归分析确定pMVR是心脏死亡(HR,0.19;95%CI,0.040 - 0.86,P = 0.031)和因心力衰竭再次住院(HR,0.28;95%CI,0.077 - 0.99,P = 0.048)的危险因素。
在FMR且LVEF≤30%的患者中,MitraClip治疗导致的围手术期并发症和死亡率低于sMVR。然而,在围手术期存活的接受手术治疗的患者,其MR残余较少,在1年时因心力衰竭再次住院的发生率较低,在1年和3年随访时心脏死亡率也低于接受pMVR治疗的患者。