"Health Shandong" Major Social Risk Prediction and Governance Collaborative Innovation Center, School of Public Health and Management, Weifang Medical University, No.7166 Baotong Xi Street, Weicheng District, Weifang, 261053, China.
Chinese Center for Disease Control and Prevention, No.27 Nanwei Road, Xicheng District, Beijing, 100050, China.
BMC Cardiovasc Disord. 2020 May 24;20(1):243. doi: 10.1186/s12872-020-01530-0.
Ischemic heart disease (IHD) is the leading cause of premature death which poses public health challenges worldwide. Previous studies focused on the overall population in China. However, variations in temporal and spatial patterns across subgroups remain unknown. This study was to analyze how the IHD burden among Chinese and subgroup populations changes in response to temporal and spatial trends from 1990 to 2016.
Based on data from the updated estimate in the 2016 Global Burden of Disease (GBD) study, we used years lived with disability (YLDs), years of life lost (YLLs), and disability-adjusted life years (DALYs) to describe the IHD burden. The percentage and annual average percentage changes were applied to illustrate temporal and spatial variations of the IHD burden stratified by age, sex, and province, over the periods 1990-2016, 1990-2005, and 2005-2016. We estimate population-attributable fraction (PAF) for 24 modifiable risk factors at the provincial level in 2016.
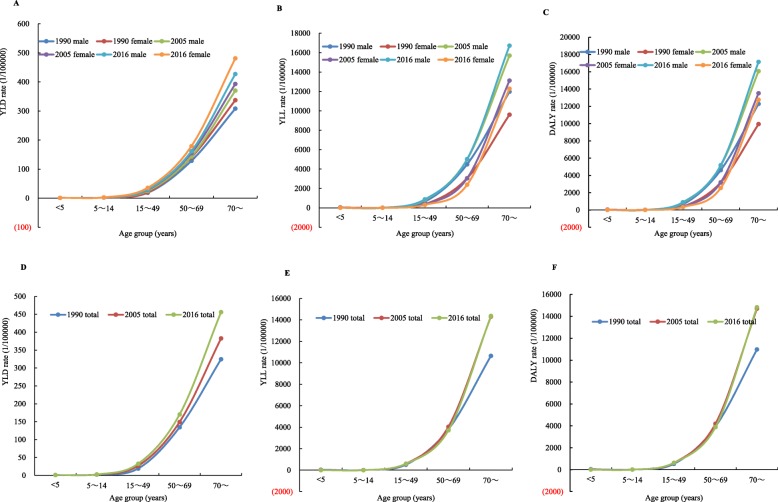
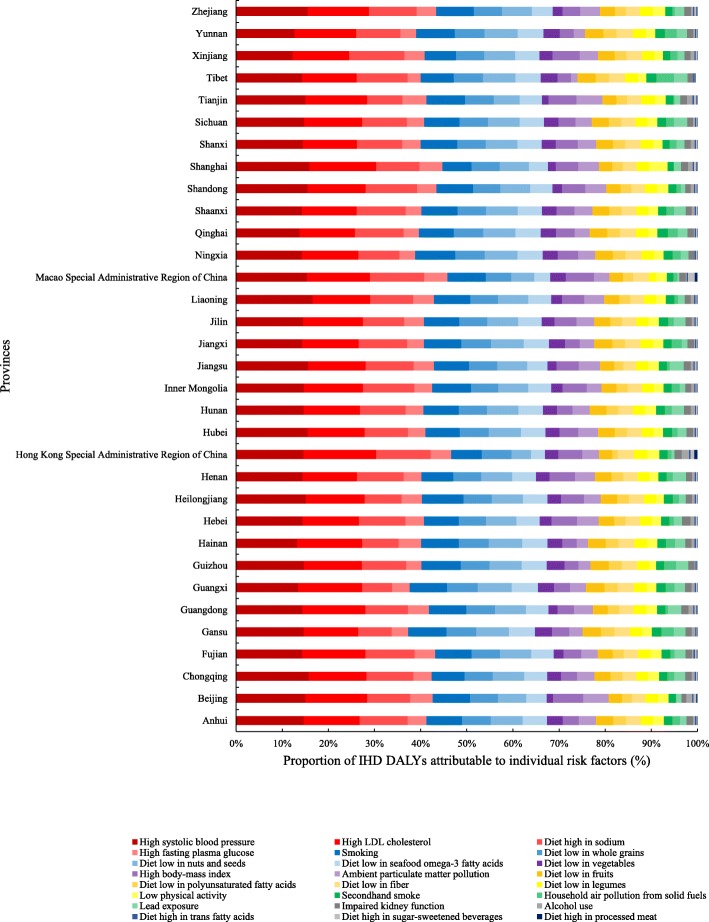
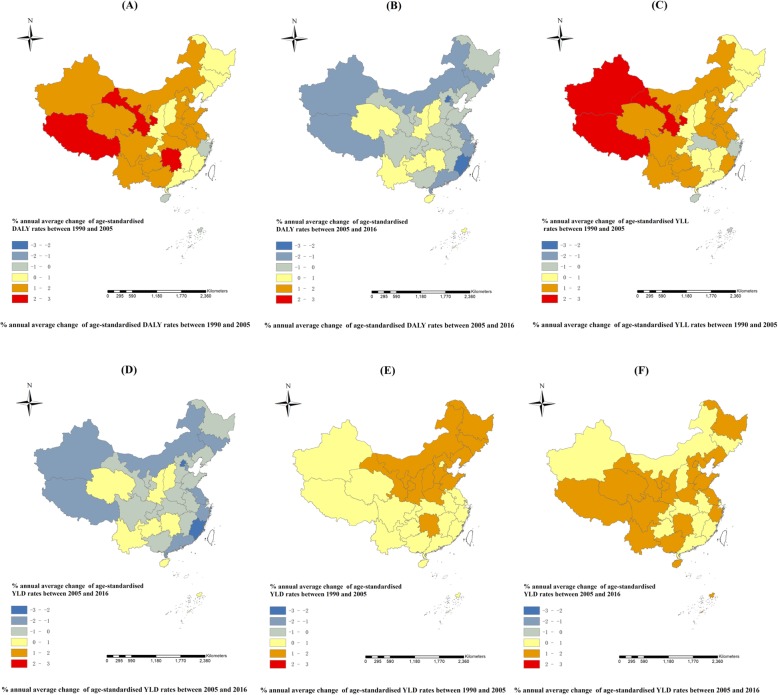
YLD rates, YLL rates, and DALY rates for IHD underwent a notable increase among all age groups and increased by 119.4, 83.3, and 84.5% nationally from 1990 to 2016. In YLD rates, a greater increase was seen in females (124.4%) compared to males (114.0%), while males experienced a more substantial increase than that in females in YLL rates (99.3% vs. 60.5%) and DALY rates (99.7% vs. 63.2%) from 1990 to 2016. Compared with 1990-2005, annual average changes in the overall population in YLL rates (3.5% vs. 1.8%) and DALY rates (3.5% vs. 1.9%) showed a tardier increase whereas an opposite increasing trend of YLD rates (3.5% vs. 4.0%) was observed between 2005 and 2016. Geographically, all provinces saw declines in the YLLs/YLDs ratio from 2005 to 2016, with seventeen of thirty-three provinces showing an upward trend between 1990 and 2005. Most provinces witnessed a remarkable upsurge in the age-standardised DALY rate from 1990 to 2016 whereas the economically advantaged region Macao (52.2%) saw the most marked reduction. High systolic blood pressure and high LDL cholesterol remained the two leading risk factors of IHD in all provinces in 2016. Diet high in sodium was the leading behavioral risks in twenty-eight provinces with smoking heading the list in five provinces.
China has made significant achievements in preventing premature death from IHD along with the increased risk of disability. Substantial disparities in temporal and spatial trends of the IHD burden emphasize concerns for elderly men and those in economically disadvantaged regions with resource constraints. Regional differences in the IHD burden can be partly explained by modifiable risk factors. By having identified these disparities, targeted IHD prevention and control strategies will help to bridge these gaps.
缺血性心脏病(IHD)是导致全球人口过早死亡的主要原因,对公共卫生构成挑战。之前的研究集中在中国的整体人口。然而,不同亚组人群的时空模式变化仍不清楚。本研究旨在分析 1990 年至 2016 年期间,中国和亚组人群的 IHD 负担如何随时间和空间趋势变化。
基于更新的 2016 年全球疾病负担(GBD)研究数据,我们使用失能生命年(YLDs)、生命损失年(YLLs)和伤残调整生命年(DALYs)来描述 IHD 负担。1990-2016 年、1990-2005 年和 2005-2016 年期间,我们使用年龄、性别和省份分层的百分比和年平均百分比变化来描述 IHD 负担的时空变化。我们估计了 2016 年省级 24 个可改变风险因素的人群归因分数(PAF)。
1990 年至 2016 年,所有年龄组的 IHD 的 YLD 率、YLL 率和 DALY 率均显著上升,全国分别上升了 119.4%、83.3%和 84.5%。在 YLD 率方面,女性(124.4%)的增幅大于男性(114.0%),而男性在 YLL 率(99.3%对 60.5%)和 DALY 率(99.7%对 63.2%)方面的增幅大于女性。与 1990-2005 年相比,2005-2016 年,总人口的 YLL 率(3.5%对 1.8%)和 DALY 率(3.5%对 1.9%)的年平均变化呈较慢增长趋势,而 YLD 率的上升趋势相反(3.5%对 4.0%)。在地理上,所有省份的 YLLs/YLDs 比值从 2005 年到 2016 年都有所下降,33 个省份中有 17 个在 1990 年至 2005 年期间呈上升趋势。1990 年至 2016 年,大多数省份的年龄标准化 DALY 率显著上升,而经济发达地区澳门(52.2%)的下降幅度最大。高收缩压和高 LDL 胆固醇仍然是 2016 年所有省份的两个主要 IHD 风险因素。在 28 个省份中,高钠饮食是主要的行为风险因素,而在 5 个省份中,吸烟是主要的风险因素。
中国在预防 IHD 导致的过早死亡方面取得了显著成就,同时残疾风险也有所增加。IHD 负担的时空趋势存在显著差异,这强调了老年人和经济贫困地区男性的问题,这些地区资源有限。IHD 负担的区域差异部分可以用可改变的风险因素来解释。通过识别这些差异,可以制定有针对性的 IHD 预防和控制策略,帮助缩小这些差距。