Department of Internal Medicine, Catholic University of Health and Allied Sciences, Mwanza, Tanzania.
Department of Internal Medicine, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania.
BMC Neurol. 2020 May 25;20(1):206. doi: 10.1186/s12883-020-01793-2.
Stroke burden in young adults is growing associated with unique risk factors and devastating outcomes. We aimed to investigate the magnitude, risk factors and outcomes of first ever stroke in young adults ≤45 years compared to older adults > 45 years.
All patients with a World Health Organization clinical definition of stroke at a tertiary hospital in Tanzania were enrolled. The National Institute of Health Stroke Scale and Modified Rankin Scale were used to assess admission stroke severity and outcomes respectively. Kaplan-Meier analysis was used to describe survival and Cox-proportional hazards model was used to examine predictors of fatality.
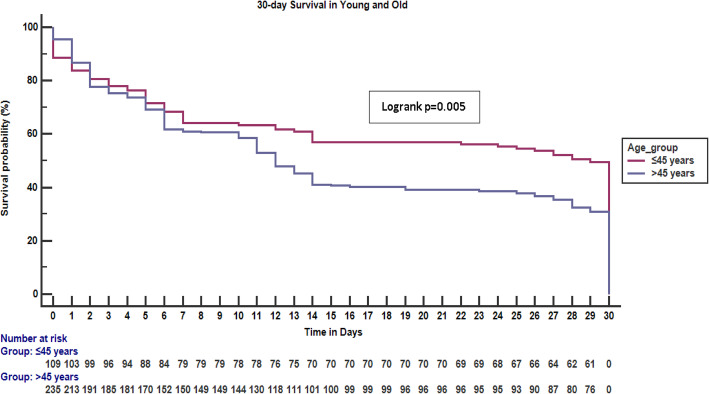
We enrolled 369 first ever stroke participants over 8 months. First strokes accounted for one quarter of the medical admissions in both younger and older groups, 123/484 {(25.4%) [95% CI 21.5-29.3%]} and 246/919 {(26.8%) [95% CI 23.9-29.6%]} respectively. Hemorrhagic stroke occurred in 47 (42.3%) vs 62 (27.2%) for the young and old respectively p = 0.005. Factors associated with stroke in the young were: a new diagnosis of hypertension in 33 (26.8%) vs 23 (9.3%) p < 0.001, HIV infection 12 (9.8%) vs 7 (2.8%) p = 0.005, use of hormonal contraception in females 33 (48.5%) vs 13 (9.4%) p < 0.001, elevated serum low density lipoproteins 28 (27.7%) vs 29 (16.4%) p = 0.024, hypercholesteremia 34 (31.2%) vs 40 (20.2%), p = 0.031, sickle cell disease 11 (9.7%) vs 9 (4.2%) p = 0.047 and thrombocytosis 12 (16.9%) vs 8 (5.6%) p = 0.007. The overall 30-day fatality rate was 215 (61.3%); 57 (49.1%) vs 158 (67.2%) in the young and old respectively. Independent predictors of fatality were: severe stroke {HR 10.35 (95% CI: 1.397-76.613)}, leukocytosis {HR 2.23 (95% CI: 1.448-3.419)} and fever {HR 1.79 (95% CI: 1.150-2.776)}.
There is a high burden of stroke in young adults that is coupled with a high 30-day fatality rate. Screening and management of hypertension is crucial in the prevention of stroke. More research is needed to identify factors which cause death, allowing the development of sustainable interventions to reduce early post stroke fatality in this group.
年轻人中风的负担正在增加,与独特的风险因素和毁灭性的后果有关。我们旨在研究首次在≤45 岁的年轻人中与>45 岁的老年人相比的中风的严重程度、风险因素和结果。
在坦桑尼亚的一家三级医院,所有符合世界卫生组织临床定义的中风患者均被纳入研究。采用国立卫生研究院中风量表和改良 Rankin 量表分别评估入院时的中风严重程度和结果。Kaplan-Meier 分析用于描述生存情况,Cox 比例风险模型用于检验死亡率的预测因素。
我们在 8 个月内纳入了 369 例首次中风患者。首次中风在年轻和老年组中的医疗入院人数中各占四分之一,分别为 123/484(25.4%)[95%CI 21.5-29.3%]和 246/919(26.8%)[95%CI 23.9-29.6%]。出血性中风在年轻人中的发生率为 47(42.3%),而老年人为 62(27.2%),p=0.005。年轻人中与中风相关的因素包括:新诊断的高血压 33 例(26.8%),23 例(9.3%),p<0.001,HIV 感染 12 例(9.8%),7 例(2.8%),p=0.005,女性使用激素避孕药 33 例(48.5%),13 例(9.4%),p<0.001,血清低密度脂蛋白升高 28 例(27.7%),29 例(16.4%),p=0.024,高胆固醇血症 34 例(31.2%),40 例(20.2%),p=0.031,镰状细胞病 11 例(9.7%),9 例(4.2%),p=0.047,血小板增多症 12 例(16.9%),8 例(5.6%),p=0.007。总的 30 天死亡率为 215(61.3%);年轻人为 57(49.1%),老年人为 158(67.2%)。死亡率的独立预测因素包括:严重中风[HR 10.35(95%CI:1.397-76.613)]、白细胞增多[HR 2.23(95%CI:1.448-3.419)]和发热[HR 1.79(95%CI:1.150-2.776)]。
年轻人中风负担沉重,30 天死亡率较高。筛查和管理高血压对于预防中风至关重要。需要进一步研究以确定导致死亡的因素,从而制定可持续的干预措施,以降低该人群中风后的早期死亡率。