Department of Internal Medicine, Catholic University of Health and Allied Sciences, P. O Box 1464, Mwanza, Tanzania.
Department of Cardiology, Jakaya Kikwete Cardiac Institute, Dar es Salaam, Tanzania.
BMC Neurol. 2020 Jul 7;20(1):270. doi: 10.1186/s12883-020-01853-7.
Stroke mimics account for up to one-third of acute stroke admissions and are a heterogeneous entity which pose diagnostic challenges. Diagnosing such patients is however crucial to avoid delays in treatment and potentially harmful medication prescription. We aimed at describing the magnitude, clinical characteristics and short-term outcomes of stroke mimics in patients clinically diagnosed with a stroke.
This prospective study enrolled patients admitted with a World Health Organization clinical criteria for stroke at a tertiary hospital in Tanzania. Baseline data was collected and the simplified version of the FABS scale was used to determine its usefulness in predicting stroke mimics. The National Institute of Health Stroke Scale and Modified Rankin Scale were used to assess for admission stroke severity and outcomes respectively.
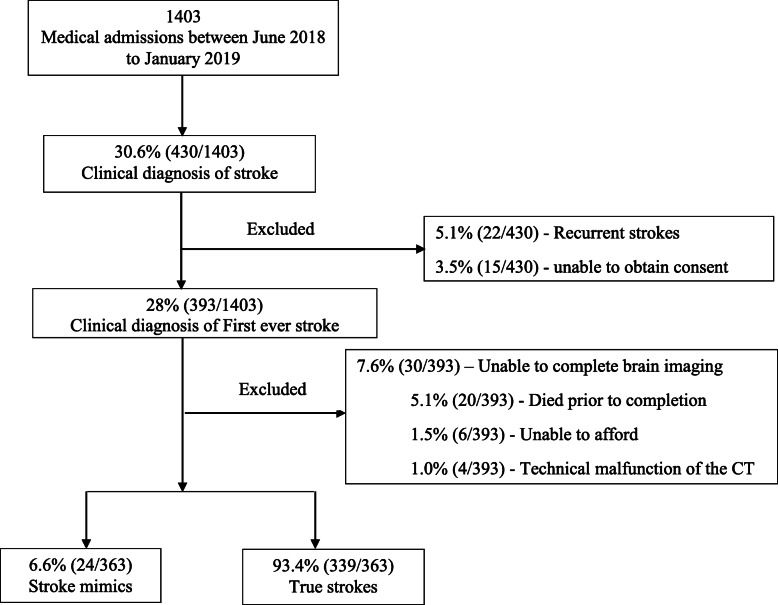
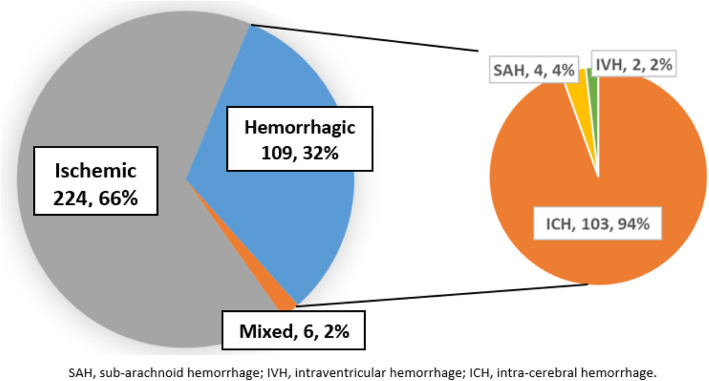
Among 363 patients with suspected stroke on admission, the final diagnosis was stroke mimics in 24 (6.6%) who had a mean age of 65.8 ± 15 years. Patients with stroke mimics were less likely to have cardiovascular risk factors for stroke including premorbid hypertension (7 (29.2%) vs 263 (77.6%), p < 0.001) and increased waist-hip ratio (9 (37.5%) vs 270 (79.6%) p < 0.001) for mimics and true strokes respectively. Clinical findings such as hypertension and the presence of cortical features in neurological examination occurred less in patients with stroke mimics. The simplified FABS score of ≥3 could identify patients with stroke mimics with a sensitivity and specificity of 38 and 80% respectively. The most common causes of mimics were brain tumors 6 (25%), meningoencephalitis 4 (16.7%) and epileptic seizures 3 (12.5%). The majority of patients with stroke mimics had severe disease on admission and the 30-day mortality in these patients was 54.5%.
In the present study, the proportion of stroke mimics among patients clinically diagnosed with stroke was 6.6% and brain tumors was a common etiology. Stroke mimics were less likely to have cardiovascular risk factors and cortical signs during evaluation. We recommend further studies that can help develop clinical scales used for predicting stroke mimics in an African population.
中风模拟占急性中风入院患者的三分之一,是一种具有诊断挑战性的异质实体。然而,诊断这些患者对于避免治疗延误和潜在有害药物处方至关重要。我们旨在描述临床上诊断为中风的患者中风模拟的程度、临床特征和短期结局。
这项前瞻性研究纳入了坦桑尼亚一家三级医院根据世界卫生组织临床标准诊断为中风的患者。收集基线数据,并使用简化版 FABS 量表来确定其预测中风模拟的有用性。国立卫生研究院中风量表和改良 Rankin 量表分别用于评估入院时的中风严重程度和结局。
在 363 名入院时疑似中风的患者中,最终诊断为中风模拟的有 24 例(6.6%),平均年龄为 65.8±15 岁。中风模拟患者发生中风的心血管危险因素较少,包括既往高血压(7 例[29.2%]与 263 例[77.6%],p<0.001)和增加的腰臀比(9 例[37.5%]与 270 例[79.6%],p<0.001)。在中风模拟患者中,临床发现如高血压和神经检查中的皮质特征较少见。简化 FABS 评分≥3 可识别中风模拟患者,其灵敏度和特异性分别为 38%和 80%。模拟患者最常见的病因是脑肿瘤 6 例(25%)、脑膜脑炎 4 例(16.7%)和癫痫发作 3 例(12.5%)。大多数中风模拟患者入院时病情严重,这些患者的 30 天死亡率为 54.5%。
在本研究中,临床上诊断为中风的患者中中风模拟的比例为 6.6%,脑肿瘤是常见的病因。中风模拟患者发生心血管危险因素和皮质体征的可能性较小。我们建议进行进一步的研究,以帮助开发用于预测非洲人群中风模拟的临床量表。