Wolfson Centre for the Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, England.
JAMA Neurol. 2020 Aug 1;77(8):947-954. doi: 10.1001/jamaneurol.2020.1326.
Asymptomatic intracranial stenosis (ICS) is a frequent finding on imaging results, particularly in the assessment of acute stroke. Although the management of symptomatic ICS is informed by randomized trials, to our knowledge there are few data on the prevalence and prognosis of asymptomatic ICS in patients with stroke and transient ischemic attack (TIA).
To study the age-specific prevalence and prognosis of asymptomatic ICS in a population-based cohort of patients with TIA and minor stroke.
DESIGN, SETTING, AND PARTICIPANTS: All patients (predominantly white) recruited to the Oxford Vascular Study (Oxfordshire, England) between March 1, 2011, and March 1, 2018, with TIA and minor ischemic stroke (National Institutes of Health Stroke Scale score, ≤3), irrespective of age, were included (n = 1579). We determined the age-specific prevalence of 50% or more asymptomatic ICS and the associated stroke risk by face-to-face follow-up to 2018 on standard medical treatment without stenting.
Patients underwent magnetic resonance angiography of the intracranial and cervicocranial arteries, computed tomography angiography if magnetic resonance angiography was contraindicated, or carotid/transcranial Doppler ultrasonography if computed tomography angiography was contraindicated.
The primary outcomes were the prevalence and prognosis of asymptomatic ICS.
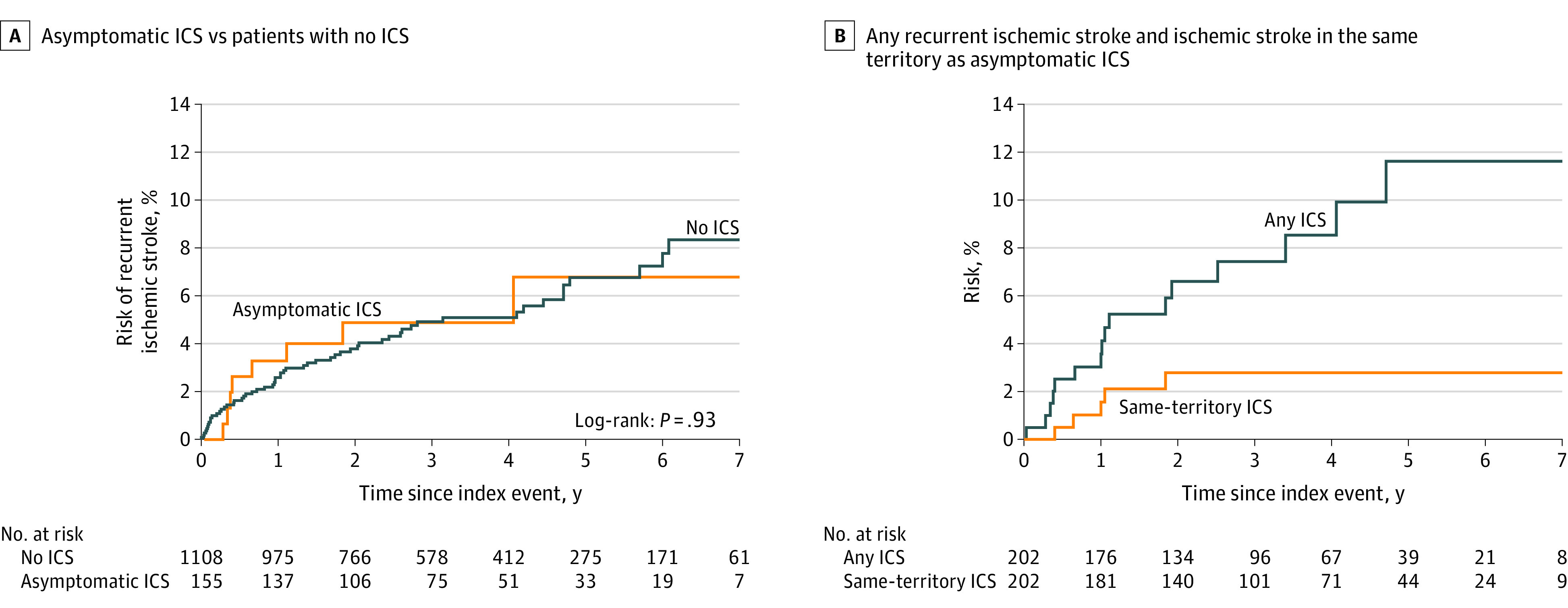
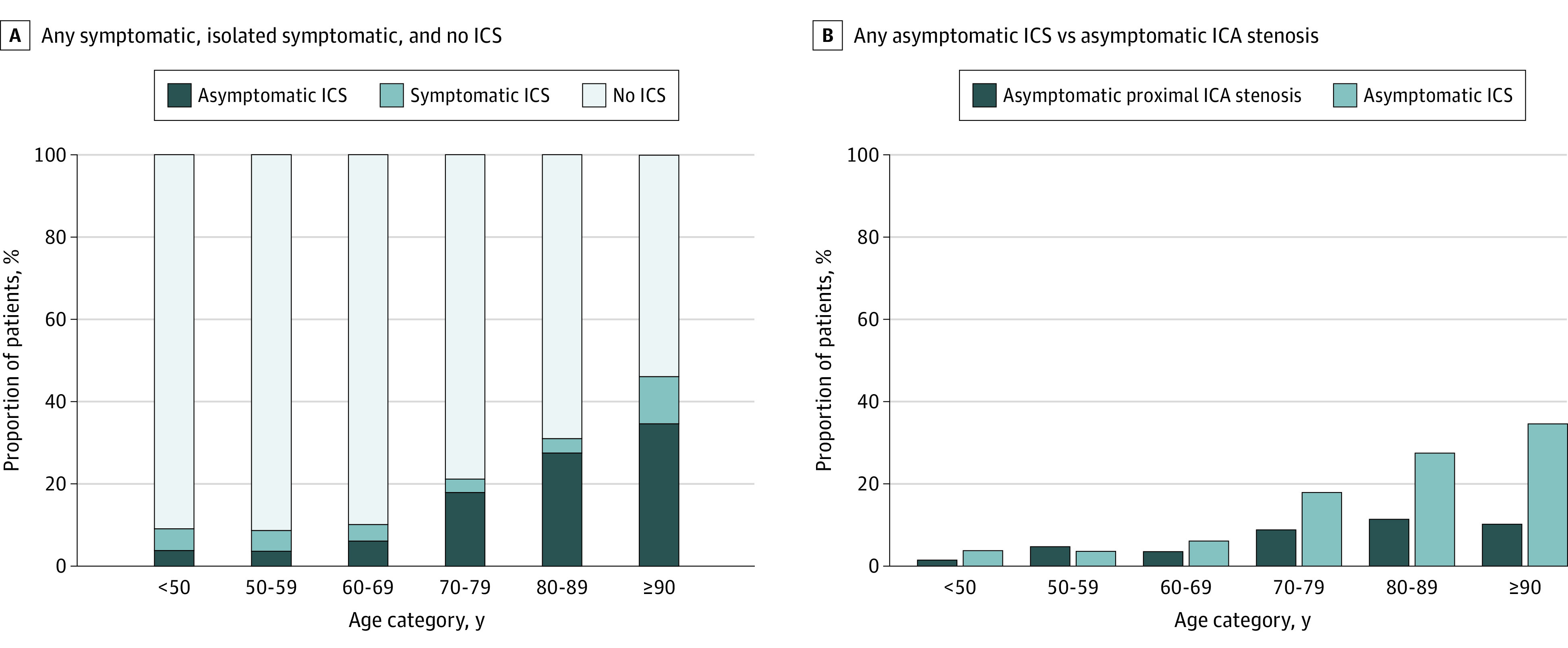
Of 1368 eligible patients (mean [SD] age, 69.2 [13.9] years; 700 men [51.2%]) with intracranial vascular imaging, 426 ICS were identified in 260 patients (19.0%): 58 (4.2%) with only symptomatic ICS, 155 (11.3%) with only asymptomatic ICS, and 47 (3.4%) with both. The prevalence of any asymptomatic ICS increased from 4.8% for patients younger than 70 years to 34.6% for patients 90 years or older (P for trend < .001; odds ratio per decade, 1.96; 95% CI, 1.69-2.27) and was greater than that of 50% or more asymptomatic carotid bifurcation stenosis (202 [14.8%] vs 105 patients [7.2%]; relative risk, 2.04; 95% CI, 1.63-2.55, P < .001). However, the 155 patients with only asymptomatic ICS had no increase in risk of ischemic stroke compared with those with no ICS (unadjusted HR, 1.03, 95% CI, 0.49-2.17), with 8 first recurrent events (5.2%) during 506 patient-years of follow-up and 3 in the territory of the ICS (annualized risk, 0.59%; 95% CI, 0.12-1.73).
The prevalence of asymptomatic ICS increases with age in white patients with TIA and minor stroke and is greater than that of asymptomatic carotid stenosis, but asymptomatic ICS does not increase the short- or medium-term risk of distal recurrent ischemic stroke for patients receiving standard medical treatment.
无症状性颅内狭窄(ICS)是影像学检查结果中的常见发现,尤其是在急性脑卒中的评估中。尽管有随机试验为症状性 ICS 的管理提供了依据,但据我们所知,在患有脑卒中或短暂性脑缺血发作(TIA)的患者中,无症状性 ICS 的患病率和预后的数据很少。
在 TIA 和小脑卒中的基于人群的队列中,研究无症状性 ICS 的年龄特异性患病率和预后。
设计、地点和参与者:所有(主要为白人)患者均纳入牛津血管研究(英格兰牛津郡),纳入时间为 2011 年 3 月 1 日至 2018 年 3 月 1 日,包括 TIA 和小缺血性脑卒中(美国国立卫生研究院脑卒中量表评分,≤3),不论年龄大小(n=1579)。我们通过标准的药物治疗(无支架)进行面对面随访至 2018 年,确定无症状性 ICS 占 50%或更多的年龄特异性患病率,以及相关的脑卒中风险。
患者接受了颅内和颅颈血管的磁共振血管造影、如果磁共振血管造影不可行则进行计算机断层血管造影、如果计算机断层血管造影不可行则进行颈动脉/经颅多普勒超声检查。
主要结局是无症状性 ICS 的患病率和预后。
在 1368 名符合颅内血管成像条件的患者中(平均[标准差]年龄 69.2[13.9]岁,700 名男性[51.2%]),260 名患者(19.0%)中发现了 426 例 ICS:58 例(4.2%)为仅有症状性 ICS,155 例(11.3%)为仅有无症状性 ICS,47 例(3.4%)为同时存在两种情况。任何无症状性 ICS 的患病率从 70 岁以下患者的 4.8%增加到 90 岁以上患者的 34.6%(趋势 P<0.001;每十年的优势比,1.96;95%置信区间,1.69-2.27),且高于 50%或更多无症状性颈动脉分叉狭窄的患病率(202 例[14.8%]比 105 例[7.2%];相对风险,2.04;95%置信区间,1.63-2.55,P<0.001)。然而,155 例仅有无症状性 ICS 的患者与无 ICS 的患者相比,其缺血性脑卒中风险没有增加(未调整的 HR,1.03,95%置信区间,0.49-2.17),506 患者-年的随访中发生了 8 例首次复发性事件(5.2%),3 例发生在 ICS 区域(年复发风险,0.59%;95%置信区间,0.12-1.73)。
在患有 TIA 和小脑卒中的白人患者中,无症状性 ICS 的患病率随年龄增长而增加,且高于无症状性颈动脉狭窄,但在接受标准药物治疗的患者中,无症状性 ICS 并不会增加远端复发性缺血性脑卒中的短期或中期风险。