Division of Cardiology University of Washington Seattle WA.
Department of Health Services University of Washington Seattle WA.
J Am Heart Assoc. 2020 Jun 2;9(11):e015317. doi: 10.1161/JAHA.119.015317. Epub 2020 May 27.
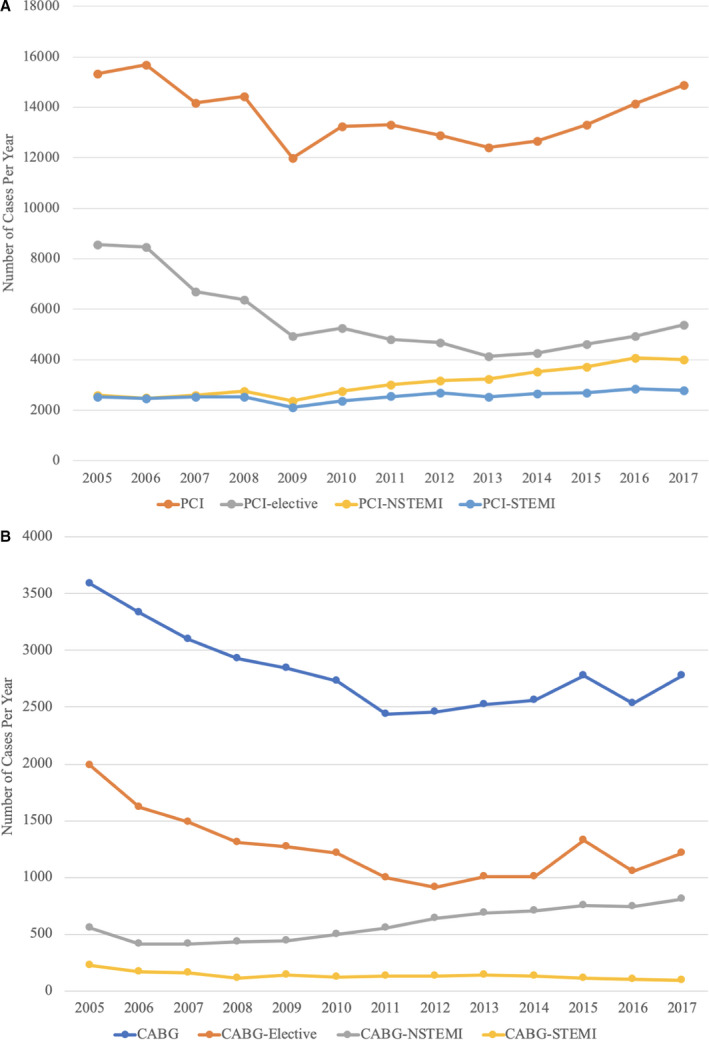
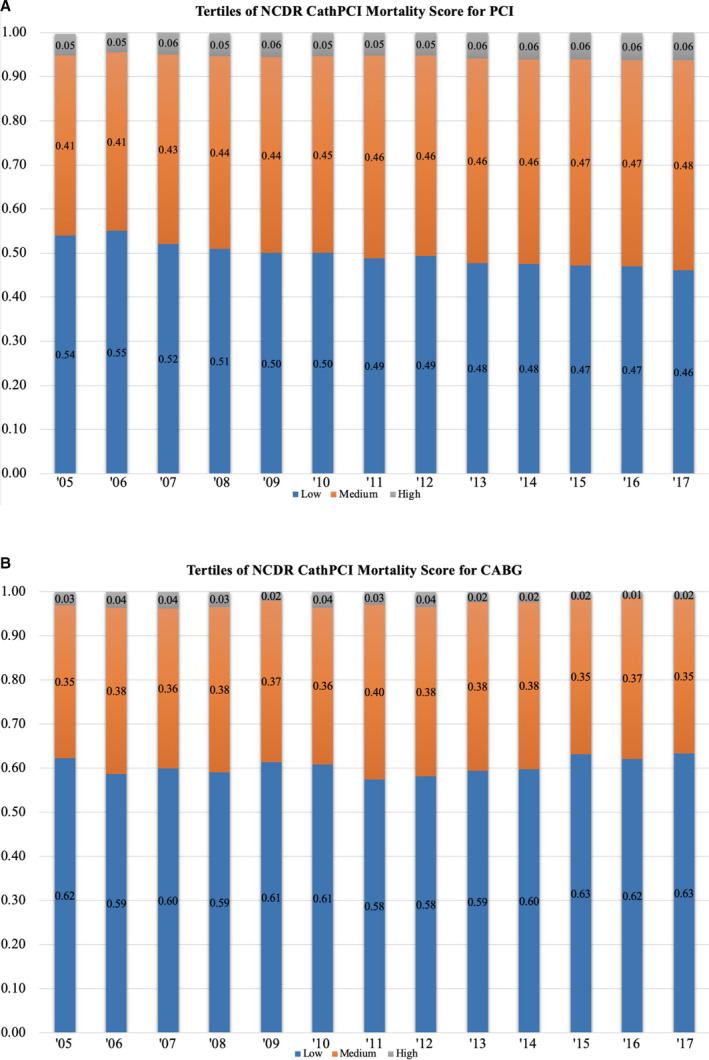
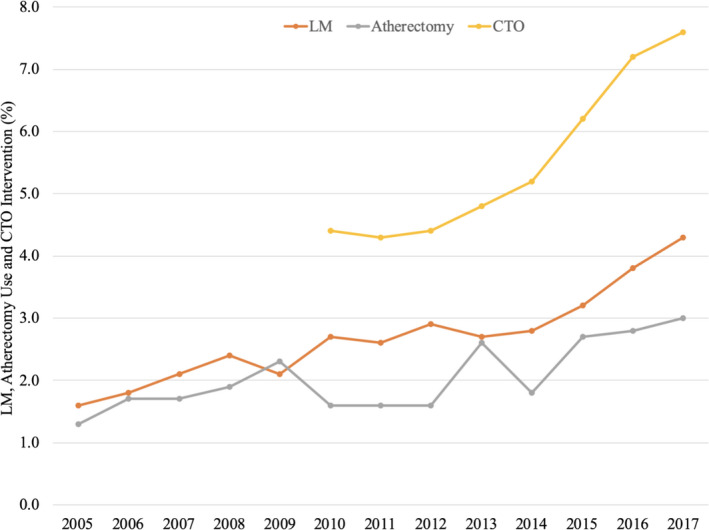
Background Patient selection and outcomes for percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG) have changed over the past decade. However, there is limited information on outcomes for both revascularization strategies in the same population. The study evaluated temporal changes in risk profile, procedural characteristics, and clinical outcomes for PCI- and CABG-treated patients. Methods and Results We analyzed all PCI and isolated CABG between 2005 and 2017 in nonfederal hospitals in Washington State. Descriptive analysis was performed to evaluate temporal changes in risk profile and, risk-adjusted in-hospital mortality. Over the study period, 178 474 PCI and 36 592 CABG procedures were performed. PCI and CABG volume decreased by 2.9% and 22.6%, respectively. Compared with 2005-2009, patients receiving either form of revascularization between 2014 and 2017 had a higher prevalence of comorbidities including diabetes mellitus and hypertension and dialysis. Presentation with ST-segment-elevation myocardial infarction (17% versus 20%) and cardiogenic shock (2.4% versus 3.4%) increased for patients with PCI compared with CABG. Conversely, clinical acuity decreased for patients receiving CABG over the study period. From 2005 to 2017, mean National Cardiovascular Data Registry CathPCI mortality score increased for patients treated with PCI (20.1 versus 22.4, <0.0001) and decreased for patients treated with CABG (18.8 versus 17.8, <0.0001). Adjusted observed/expected in-hospital mortality ratio increased for PCI (0.98 versus 1.19, <0.0001) but decreased for CABG (1.21 versus 0.74, <0.0001) over the study period. Conclusions Clinical acuity increased for patients treated with PCI rather than CABG. This resulted in an increase in adjusted observed/expected mortality ratio for patients undergoing PCI and a decrease for CABG. These shifts may reflect an increased use of PCI instead of CABG for patients considered to be at high surgical risk.
背景 经皮冠状动脉介入治疗(PCI)和冠状动脉旁路移植术(CABG)的患者选择和结果在过去十年中发生了变化。然而,关于同一人群中这两种血运重建策略的结果的信息有限。本研究评估了 PCI 和 CABG 治疗患者的风险特征、手术特征和临床结局的时间变化。
方法和结果 我们分析了 2005 年至 2017 年期间华盛顿州非联邦医院的所有 PCI 和孤立的 CABG。进行描述性分析以评估风险特征和风险调整后的住院死亡率的时间变化。在研究期间,进行了 178474 例 PCI 和 36592 例 CABG 手术。PCI 和 CABG 量分别减少了 2.9%和 22.6%。与 2005-2009 年相比,2014-2017 年接受两种血运重建方式的患者更常患有合并症,包括糖尿病和高血压以及透析。与 CABG 相比,接受 PCI 的患者 ST 段抬高型心肌梗死(17%比 20%)和心源性休克(2.4%比 3.4%)的发生率更高。相反,在研究期间,接受 CABG 的患者的临床严重程度下降。从 2005 年到 2017 年,接受 PCI 治疗的患者的国家心血管数据登记 CathPCI 死亡率评分平均值增加(20.1 比 22.4,<0.0001),接受 CABG 治疗的患者减少(18.8 比 17.8,<0.0001)。在研究期间,接受 PCI 治疗的患者的观察/预期住院死亡率比值增加(0.98 比 1.19,<0.0001),而接受 CABG 治疗的患者减少(1.21 比 0.74,<0.0001)。
结论 接受 PCI 治疗的患者的临床严重程度增加,而不是 CABG。这导致接受 PCI 的患者的调整后观察/预期死亡率比值增加,而 CABG 则减少。这些转变可能反映出考虑手术风险较高的患者对 PCI 的使用增加而对 CABG 的使用减少。