National Clinician Scholars Program, Corporal Michael J. Crescenz Veterans Affairs Medical Center, University of Pennsylvania, Philadelphia.
Center for Emergency Care Policy and Research, Perelman School of Medicine, Department of Emergency Medicine, University of Pennsylvania, Philadelphia.
JAMA Netw Open. 2020 May 1;3(5):e205852. doi: 10.1001/jamanetworkopen.2020.5852.
Timely initiation and referral to treatment for patients with opioid use disorder seen in the emergency department is associated with reduced mortality. It is not known how often commercially insured adults obtain follow-up treatment after nonfatal opioid overdose.
To investigate the incidence of follow-up treatment following emergency department discharge after nonfatal opioid overdose and patient characteristics associated with receipt of follow-up treatment.
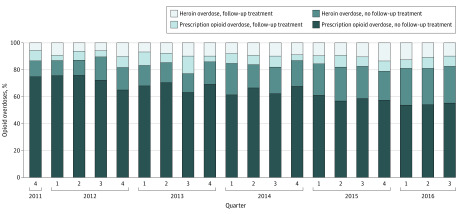
DESIGN, SETTING, AND PARTICIPANTS: A retrospective cohort study was conducted using an administrative claims database for a large US commercial insurer, from October 1, 2011, to September 30, 2016. Data analysis was performed from May 1, 2019, to September 26, 2019. Adult patients discharged from the emergency department after an index opioid overdose (no overdose in the preceding 90 days) were included. Patients with cancer and without continuous insurance enrollment were excluded.
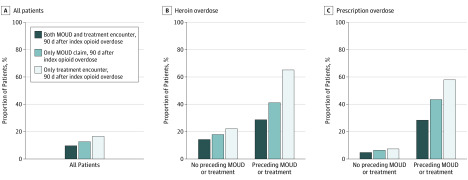
The primary outcome was follow-up treatment in the 90 days following overdose, defined as a combined outcome of claims for treatment encounters or medications for opioid use disorder (buprenorphine and naltrexone). Analysis was stratified by whether patients received treatment for opioid use disorder in the 90 days before the overdose. Logistic regression models were used to identify patient characteristics associated with receipt of follow-up treatment. Marginal effects were used to report the average adjusted probability and absolute risk differences (ARDs) in follow-up for different patient characteristics.
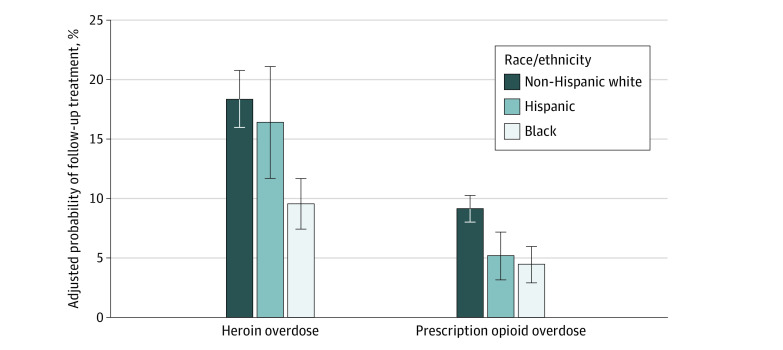
A total of 6451 patients were identified with nonfatal opioid overdose; the mean (SD) age was 45.0 (19.3) years, 3267 were women (50.6%), and 4676 patients (72.5%) reported their race as non-Hispanic white. A total of 1069 patients (16.6%; 95% CI, 15.7%-17.5%) obtained follow-up treatment within 90 days after the overdose. In adjusted analysis of patients who did not receive treatment before the overdose, black patients were half as likely to obtain follow-up compared with non-Hispanic white patients (ARD, -5.9%; 95% CI, -8.6% to -3.6%). Women (ARD, -1.7%; 95% CI, -3.3% to -0.5%) and Hispanic patients (ARD, -3.5%; 95% CI, -6.1% to -0.9%) were also less likely to obtain follow-up. For each additional year of age, patients were 0.2% less likely to obtain follow-up (95% CI, -0.3% to -0.1%).
Efforts to improve the low rate of timely follow-up treatment following opioid overdose may seek to address sex, race/ethnicity, and age disparities.
在急诊科就诊的阿片类药物使用障碍患者,如果能及时开始并转至治疗,其死亡率会降低。但目前尚不清楚,有多少商业保险的成年人在非致命性阿片类药物过量后会接受后续治疗。
调查非致命性阿片类药物过量后急诊科出院患者接受后续治疗的情况,以及与接受后续治疗相关的患者特征。
设计、地点和参与者:这是一项使用美国一家大型商业保险公司的行政索赔数据库进行的回顾性队列研究,时间为 2011 年 10 月 1 日至 2016 年 9 月 30 日。数据分析于 2019 年 5 月 1 日至 2019 年 9 月 26 日进行。纳入的是在阿片类药物过量后(前 90 天内没有过量)从急诊科出院的成年患者。排除患有癌症且没有连续保险登记的患者。
主要结局是在过量后 90 天内接受后续治疗,定义为治疗性就诊或阿片类药物使用障碍治疗药物(丁丙诺啡和纳曲酮)的索赔综合结果。分析按患者在过量前 90 天内是否接受过阿片类药物使用障碍治疗进行分层。采用 logistic 回归模型确定与接受后续治疗相关的患者特征。使用边际效应报告不同患者特征的后续治疗的平均调整概率和绝对风险差异(ARD)。
共确定了 6451 例非致命性阿片类药物过量患者;平均(SD)年龄为 45.0(19.3)岁,3267 例为女性(50.6%),4676 例患者(72.5%)报告其种族为非西班牙裔白人。共有 1069 例患者(16.6%;95%CI,15.7%-17.5%)在过量后 90 天内接受了后续治疗。在未接受过治疗的过量前患者的调整分析中,与非西班牙裔白人患者相比,黑人患者接受后续治疗的可能性低一半(ARD,-5.9%;95%CI,-8.6%至-3.6%)。女性(ARD,-1.7%;95%CI,-3.3%至-0.5%)和西班牙裔患者(ARD,-3.5%;95%CI,-6.1%至-0.9%)也不太可能接受后续治疗。每增加 1 岁,患者接受后续治疗的可能性就会降低 0.2%(95%CI,-0.3%至-0.1%)。
为提高阿片类药物过量后及时进行后续治疗的低比率而进行的努力,可能需要解决性别、种族/民族和年龄差异的问题。