Haematology Department, Nottingham University Hospitals NHS Trust, Nottingham, UK.
Cancer Research UK and UCL Cancer Trials Centre, UCL Cancer Institute, University College London, London, UK; Division of Cancer Sciences, University of Manchester and The Christie Hospital NHS Trust, Manchester, UK.
Ann Oncol. 2020 Sep;31(9):1251-1259. doi: 10.1016/j.annonc.2020.05.016. Epub 2020 May 26.
Outcomes for patients with high-risk diffuse large B-cell lymphoma (DLBCL) treated with R-CHOP chemotherapy are suboptimal but, to date, no alternative regimen has been shown to improve survival rates. This phase 2 trial aimed to assess the efficacy of a Burkitt-like approach for high-risk DLBCL using the dose-intense R-CODOX-M/R-IVAC regimen.
Eligible patients were aged 18-65 years with stage II-IV untreated DLBCL and an International Prognostic Index (IPI) score of 3-5. Patients received alternating cycles of CODOX-M (cyclophosphamide, vincristine, doxorubicin and high-dose methotrexate) alternating with IVAC chemotherapy (ifosfamide, etoposide and high-dose cytarabine) plus eight doses of rituximab. Response was assessed by computed tomography after completing all four cycles of chemotherapy. The primary end point was 2-year progression-free survival (PFS).
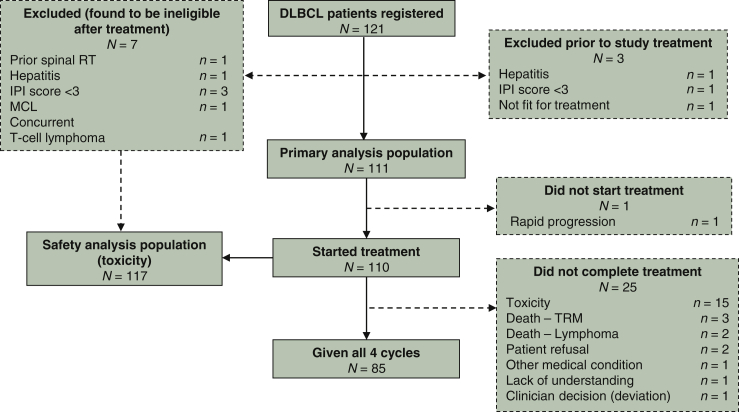
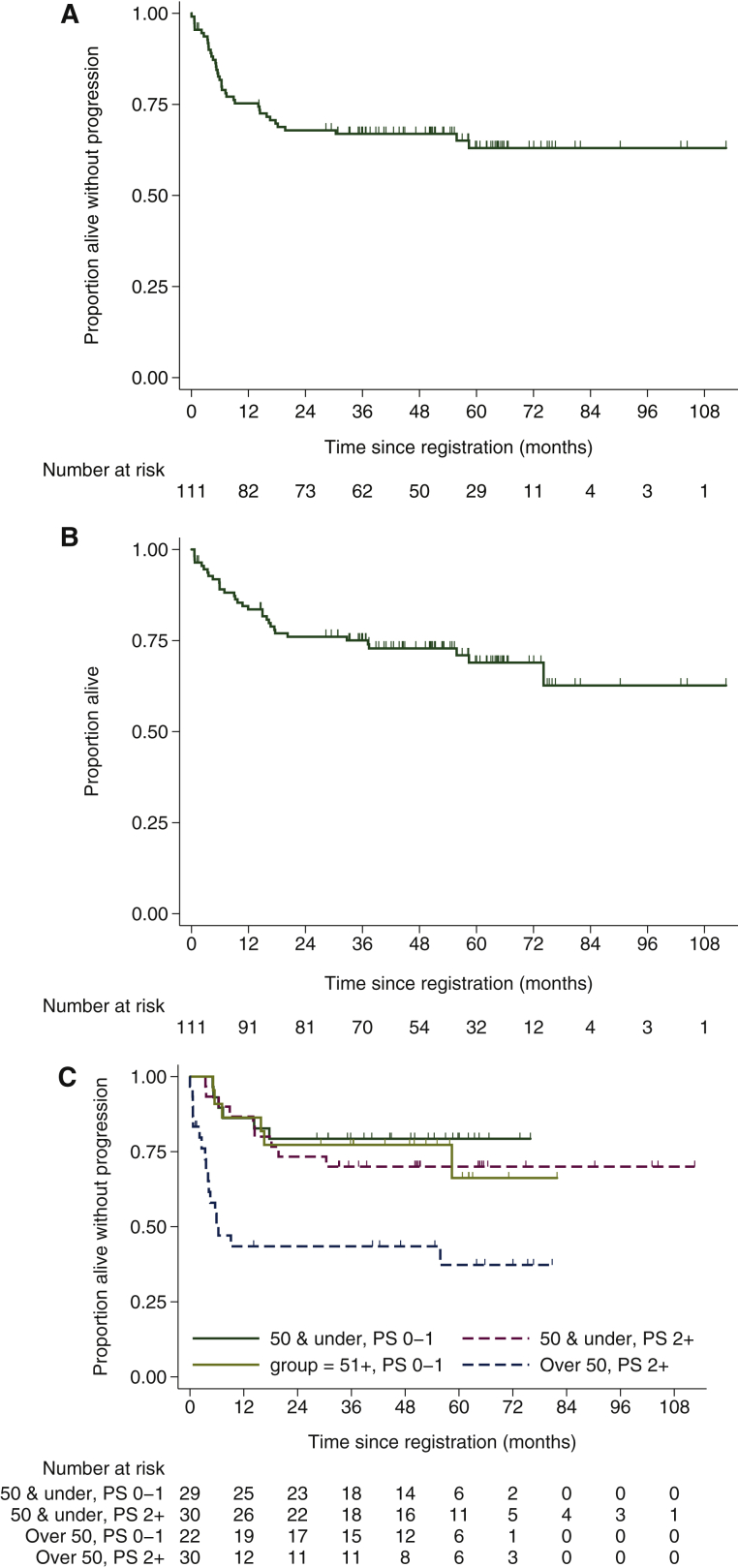
A total of 111 eligible patients were registered; median age was 50 years, IPI score was 3 (60.4%) or 4/5 (39.6%), 54% had a performance status ≥2 and 9% had central nervous system involvement. A total of 85 patients (76.6%) completed all four cycles of chemotherapy. There were five treatment-related deaths (4.3%), all in patients with performance status of 3 and aged >50 years. Two-year PFS for the whole cohort was 67.9% [90% confidence interval (CI) 59.9-74.6] and 2-year overall survival was 76.0% (90% CI 68.5-82.0). The ability to tolerate and complete treatment was lower in patients with performance status ≥2 who were aged >50 years, where 2-year PFS was 43.5% (90% CI 27.9-58.0).
This trial demonstrates that R-CODOX-M/R-IVAC is a feasible and effective regimen for the treatment of younger and/or fit patients with high-risk DLBCL. These encouraging survival rates demonstrate that this regimen warrants further investigation against standard of care.
ClinicalTrials.gov (NCT00974792) and EudraCT (2005-003479-19).
接受 R-CHOP 化疗的高危弥漫性大 B 细胞淋巴瘤(DLBCL)患者的治疗结果并不理想,但迄今为止,尚无其他方案显示能提高生存率。本 2 期试验旨在使用剂量密集型 R-CODOX-M/R-IVAC 方案评估伯基特样方案治疗高危 DLBCL 的疗效。
符合条件的患者为年龄在 18-65 岁、未经治疗的 II-IV 期 DLBCL 患者,且国际预后指数(IPI)评分为 3-5。患者接受 CODOX-M(环磷酰胺、长春新碱、多柔比星和高剂量甲氨蝶呤)与 IVAC 化疗(异环磷酰胺、依托泊苷和高剂量阿糖胞苷)交替的周期治疗,加用 8 剂利妥昔单抗。完成所有 4 个周期化疗后,通过计算机断层扫描评估反应。主要终点为 2 年无进展生存率(PFS)。
共登记了 111 例符合条件的患者;中位年龄为 50 岁,IPI 评分为 3(60.4%)或 4/5(39.6%),54%的患者体能状态≥2,9%的患者有中枢神经系统受累。85 例(76.6%)患者完成了所有 4 个周期的化疗。有 5 例治疗相关死亡(4.3%),均发生在体能状态为 3 且年龄>50 岁的患者中。全队列 2 年 PFS 为 67.9%[90%置信区间(CI)59.9-74.6],2 年总生存率为 76.0%(90%CI 68.5-82.0)。体能状态≥2 且年龄>50 岁的患者耐受性和完成治疗的能力较低,2 年 PFS 为 43.5%[90%CI 27.9-58.0]。
本试验表明,R-CODOX-M/R-IVAC 是治疗年轻和/或体能状态良好的高危 DLBCL 患者的一种可行且有效的方案。这些令人鼓舞的生存率表明,该方案值得进一步研究以替代标准治疗。
ClinicalTrials.gov(NCT00974792)和 EudraCT(2005-003479-19)。