Graduate Biomedical Sciences, University of Alabama at Birmingham, Birmingham, Alabama, United States of America.
School of Health Professions Honors Undergraduate Research Program, University of Alabama at Birmingham, Birmingham, Alabama, United States of America.
PLoS One. 2020 May 29;15(5):e0233795. doi: 10.1371/journal.pone.0233795. eCollection 2020.
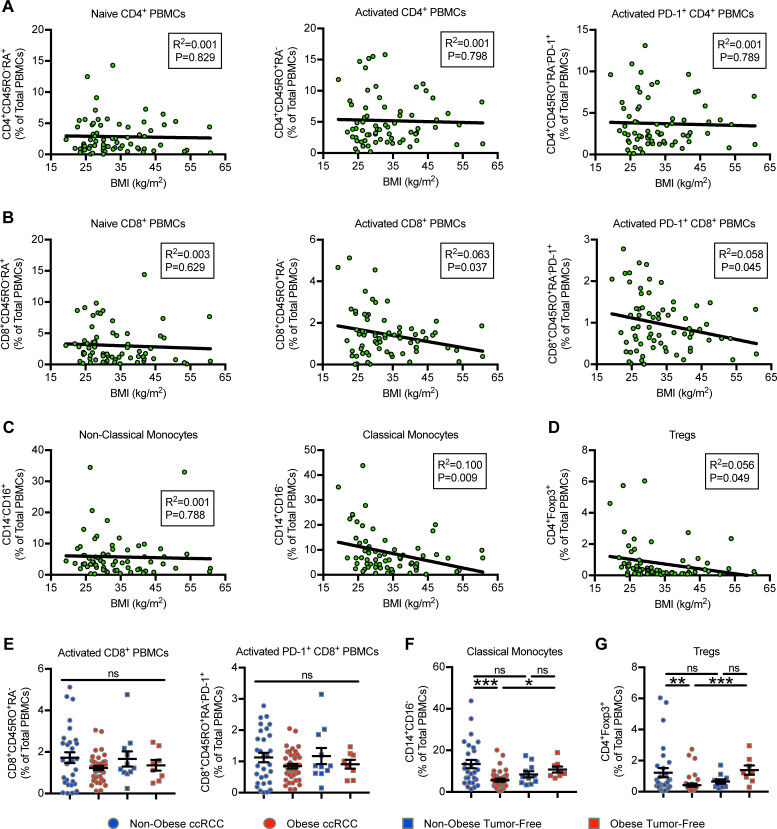
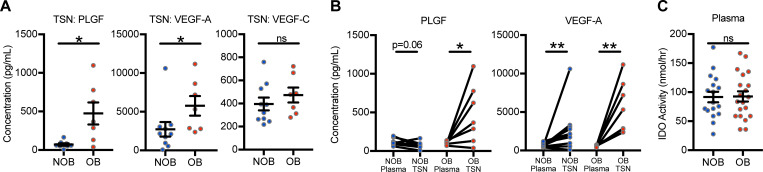
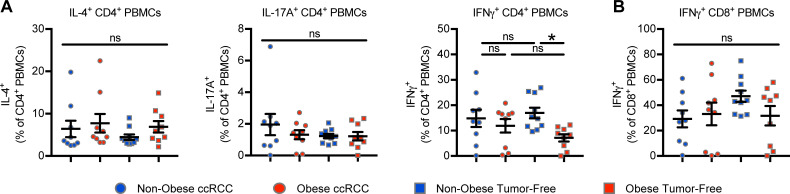
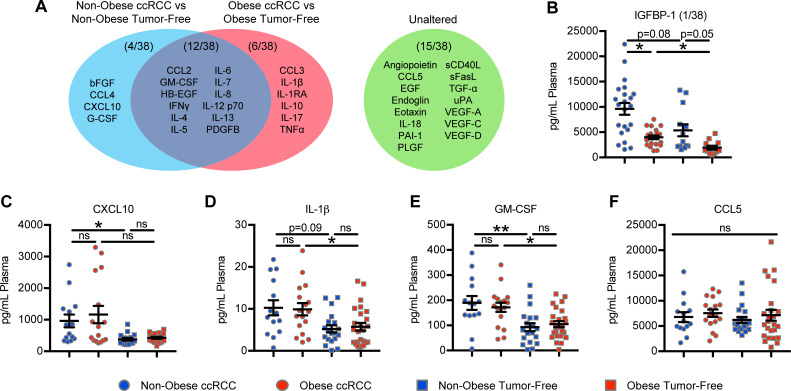
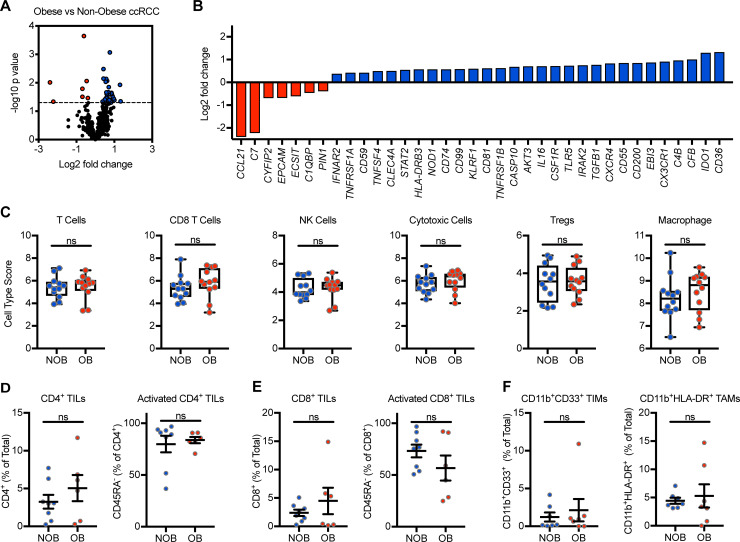
Understanding the effects of obesity on the immune profile of renal cell carcinoma (RCC) patients is critical, given the rising use of immunotherapies to treat advanced disease and recent reports of differential cancer immunotherapy outcomes with obesity. Here, we evaluated multiple immune parameters at the genetic, soluble protein, and cellular levels in peripheral blood and renal tumors from treatment-naive clear cell RCC (ccRCC) subjects (n = 69), to better understand the effects of host obesity (Body Mass Index "BMI" ≥ 30 kg/m2) in the absence of immunotherapy. Tumor-free donors (n = 38) with or without obesity were used as controls. In our ccRCC cohort, increasing BMI was associated with decreased percentages of circulating activated PD-1+CD8+ T cells, CD14+CD16neg classical monocytes, and Foxp3+ regulatory T cells (Tregs). Only CD14+CD16neg classical monocytes and Tregs were reduced when obesity was examined as a categorical variable. Obesity did not alter the percentages of circulating IFNγ+ CD8 T cells or IFNγ+, IL-4+, or IL-17A+ CD4 T cells in ccRCC subjects. Of 38 plasma proteins analyzed, six (CCL3, IL-1β, IL-1RA, IL-10, IL-17, and TNFα) were upregulated specifically in ccRCC subjects with obesity versus tumor-free controls with obesity. IGFBP-1 was uniquely decreased in ccRCC subjects with obesity versus non-obese ccRCC subjects. Immunogenetic profiling of ccRCC tumors revealed that 93% of examined genes were equivalently expressed and no changes in cell type scores were found in stage-matched tumors from obesity category II/III versus normal weight (BMI ≥ 35 kg/m2 versus 18.5-24.9 kg/m2, respectively) subjects. Intratumoral PLGF and VEGF-A proteins were elevated in ccRCC subjects with obesity. Thus, in ccRCC patients with localized disease, obesity is not associated with widespread detrimental alterations in systemic or intratumoral immune profiles. The effects of combined obesity and immunotherapy administration on immune parameters remains to be determined.
了解肥胖对肾细胞癌(RCC)患者免疫谱的影响至关重要,因为免疫疗法越来越多地被用于治疗晚期疾病,而且最近有报道称肥胖会对癌症免疫疗法的结果产生差异。在这里,我们评估了来自未经治疗的透明细胞肾细胞癌(ccRCC)患者(n = 69)外周血和肾肿瘤中的多个免疫参数,包括遗传、可溶性蛋白和细胞水平,以更好地了解宿主肥胖(BMI≥30kg/m2)在没有免疫治疗的情况下对免疫的影响。使用无肥胖的肿瘤游离供体(n = 38)作为对照。在我们的 ccRCC 队列中,BMI 的增加与循环激活的 PD-1+CD8+T 细胞、CD14+CD16neg 经典单核细胞和 Foxp3+调节性 T 细胞(Tregs)的百分比降低有关。仅当将肥胖视为分类变量时,才会观察到 CD14+CD16neg 经典单核细胞和 Tregs 的减少。在 ccRCC 患者中,肥胖并未改变循环 IFNγ+CD8 T 细胞或 IFNγ+、IL-4+或 IL-17A+CD4 T 细胞的百分比。在分析的 38 种血浆蛋白中,有 6 种(CCL3、IL-1β、IL-1RA、IL-10、IL-17 和 TNFα)在肥胖的 ccRCC 患者中特异性上调,而肥胖的肿瘤游离对照中则没有。IGFBP-1 仅在肥胖的 ccRCC 患者中降低,而在肥胖的非肥胖 ccRCC 患者中则没有。ccRCC 肿瘤的免疫遗传分析显示,93%的检测基因表达水平相同,在肥胖类别 II/III 与正常体重(BMI≥35kg/m2 与 18.5-24.9kg/m2,分别)患者的匹配分期肿瘤中,未发现细胞类型评分的变化。肥胖的 ccRCC 患者肿瘤内 PLGF 和 VEGF-A 蛋白升高。因此,在局部疾病的 ccRCC 患者中,肥胖与全身或肿瘤内免疫谱的广泛不良改变无关。肥胖和免疫治疗联合应用对免疫参数的影响仍有待确定。