University of North Carolina at Chapel Hill, USA.
Health Inf Manag. 2021 Sep;50(3):107-117. doi: 10.1177/1833358320920589. Epub 2020 Jun 1.
Some physicians in intensive care units (ICUs) report that electronic health records (EHRs) can be cumbersome and disruptive to workflow. There are significant gaps in our understanding of the physician-EHR interaction.
To better understand how clinicians use the EHR for chart review during ICU pre-rounds through the characterisation and description of screen navigation pathways and workflow patterns.
We conducted a live, direct observational study of six physician trainees performing electronic chart review during daily pre-rounds in the 30-bed medical ICU at a large academic medical centre in the Southeastern United States. A tailored checklist was used by observers for data collection.
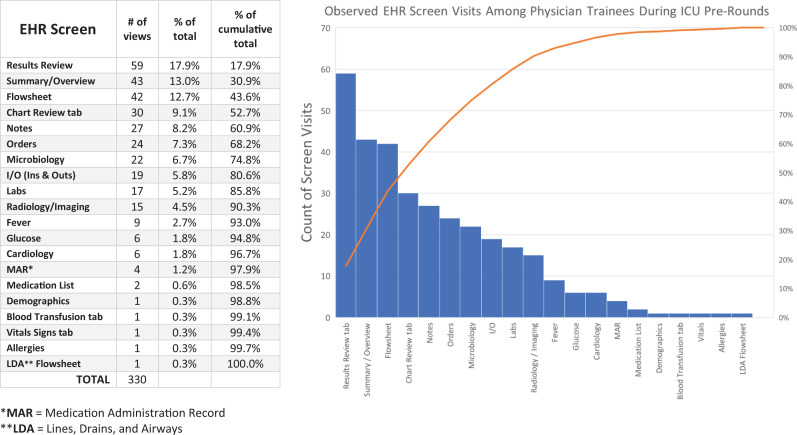
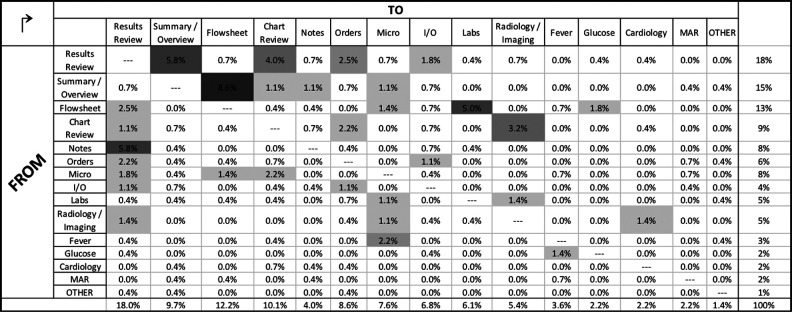
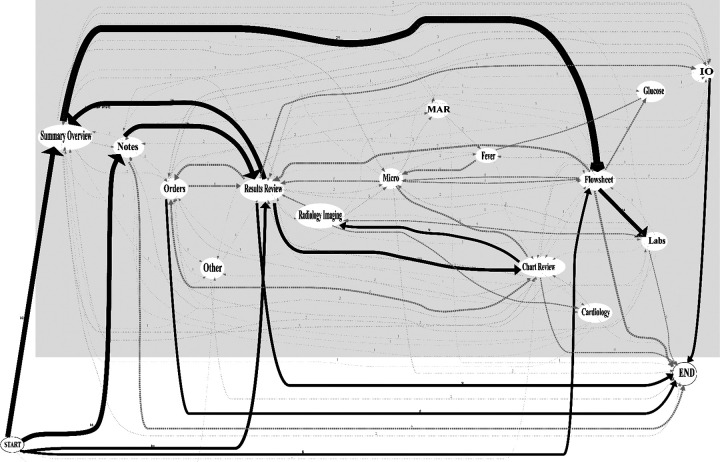
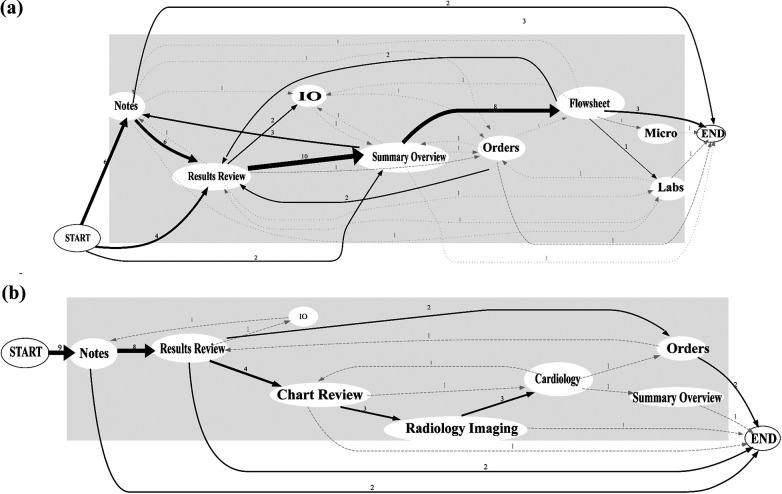
We observed 52 distinct live patient chart review encounters, capturing a total of 2.7 hours of pre-rounding chart review activity by six individual physicians. Physicians reviewed an average of 8.7 patients (range = 5-12), spending a mean of 3:05 minutes per patient (range = 1:34-5:18). On average, physicians visited 6.3 (±3.1) total EHR screens per patient (range = 1-16). Four unique screens were viewed most commonly, accounting for over half (52.7%) of all screen visits: results review (17.9%), summary/overview (13.0%), flowsheet (12.7%), and the chart review tab (9.1%). Navigation pathways were highly variable, but several common screen transition patterns emerged across users. Average interrater reliability for the paired EHR observation was 80.0%.
We observed the physician-EHR interaction during ICU pre-rounds to be brief and highly focused. Although we observed a high degree of "information sprawl" in physicians' digital navigation, we also identified common launch points for electronic chart review, key high-traffic screens and common screen transition patterns.
From the study findings, we suggest recommendations towards improved EHR design.
一些重症监护病房(ICU)的医生报告称,电子病历(EHR)可能繁琐且会中断工作流程。我们对医生与 EHR 的交互作用的理解存在很大差距。
通过描述和描述屏幕导航路径和工作流程模式,更好地了解临床医生如何在 ICU 预查房期间使用 EHR 进行病历回顾。
我们对美国东南部一家大型学术医疗中心的 30 张病床的内科重症监护病房(ICU)中进行的日常预查房期间的 6 名住院医师进行了现场直接观察研究。观察者使用定制检查表进行数据收集。
我们观察了 52 次独特的实时患者病历回顾,记录了 6 名医生总共 2.7 小时的预查房病历回顾活动。每位医生平均检查 8.7 名患者(范围= 5-12),每名患者平均花费 3:05 分钟(范围= 1:34-5:18)。每位医生平均访问 6.3(±3.1)次 EHR 总屏幕(范围= 1-16)。最常查看的是四个独特的屏幕,占所有屏幕访问量的一半以上(52.7%):结果审查(17.9%)、摘要/概述(13.0%)、流程图(12.7%)和病历审查选项卡(9.1%)。导航路径高度可变,但在用户之间出现了几种常见的屏幕转换模式。成对 EHR 观察的平均组内相关系数为 80.0%。
我们观察到 ICU 预查房期间的医生与 EHR 的交互作用是短暂而高度集中的。尽管我们在医生的数字导航中观察到了高度的“信息扩散”,但我们也确定了电子病历审查的常见启动点、关键高流量屏幕和常见的屏幕转换模式。
从研究结果中,我们提出了一些改进 EHR 设计的建议。