Yamana Ippei, Murakami Takuo, Ryu Shintaro, Ichikawa Jun, Shin Yuki, Koreeda Nobuhiko, Sannomiya Hiroto, Sato Keisuke, Okamoto Tatsuya, Sakamoto Yasuo, Yoshida Yasushi, Yanagisawa Jun, Noritomi Tomoaki, Hasegawa Suguru
Department of Surgery, Fukuoka Tokushukai Hospital, 4-5 Sukukita, Kasuga, Fukuoka, 816-0864, Japan.
Department of Surgery, Fukuoka Tokushukai Hospital, 4-5 Sukukita, Kasuga, Fukuoka, 816-0864, Japan.
Int J Surg Case Rep. 2020;71:290-293. doi: 10.1016/j.ijscr.2020.04.049. Epub 2020 May 11.
Currently, the frequency of evaluating the flow of a reconstructed gastric tube using indocyanine green (ICG) fluorescence has been increasing. However, it has been difficult to decide on the operation method for patients with gastric tube cancer (GTC). We herein report a case in which ICG was effective in a patient with resection of GTC.
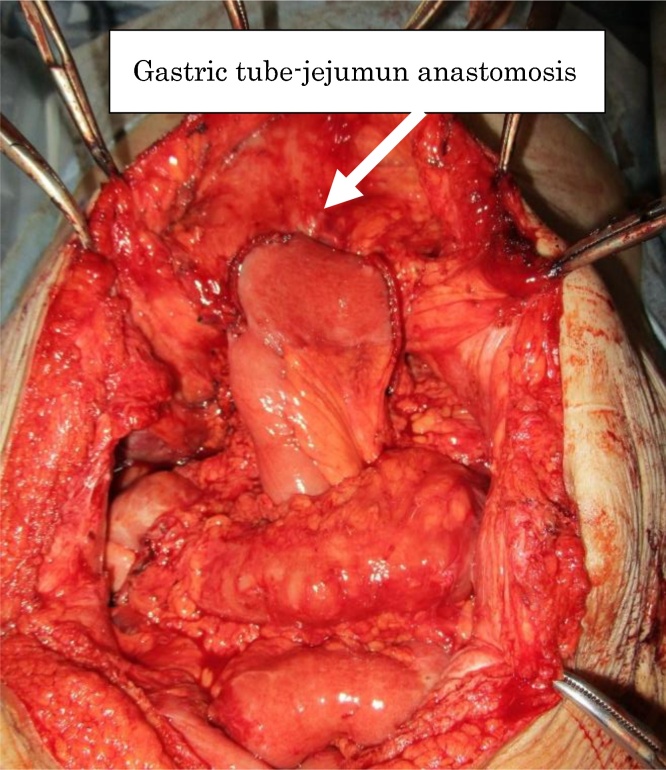
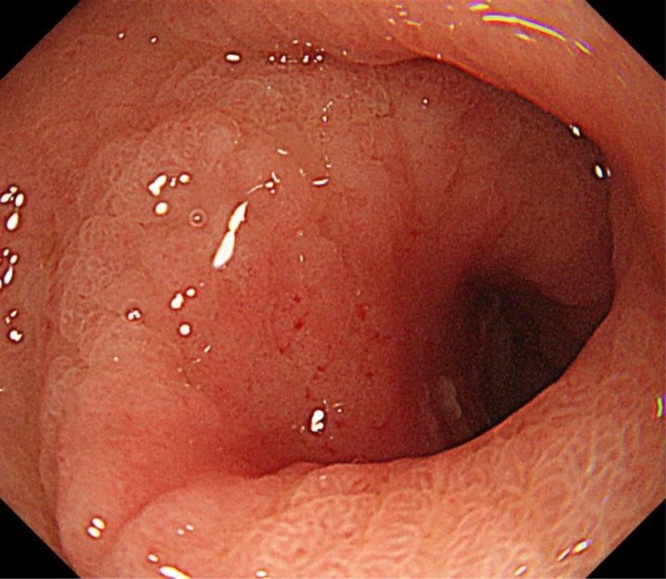
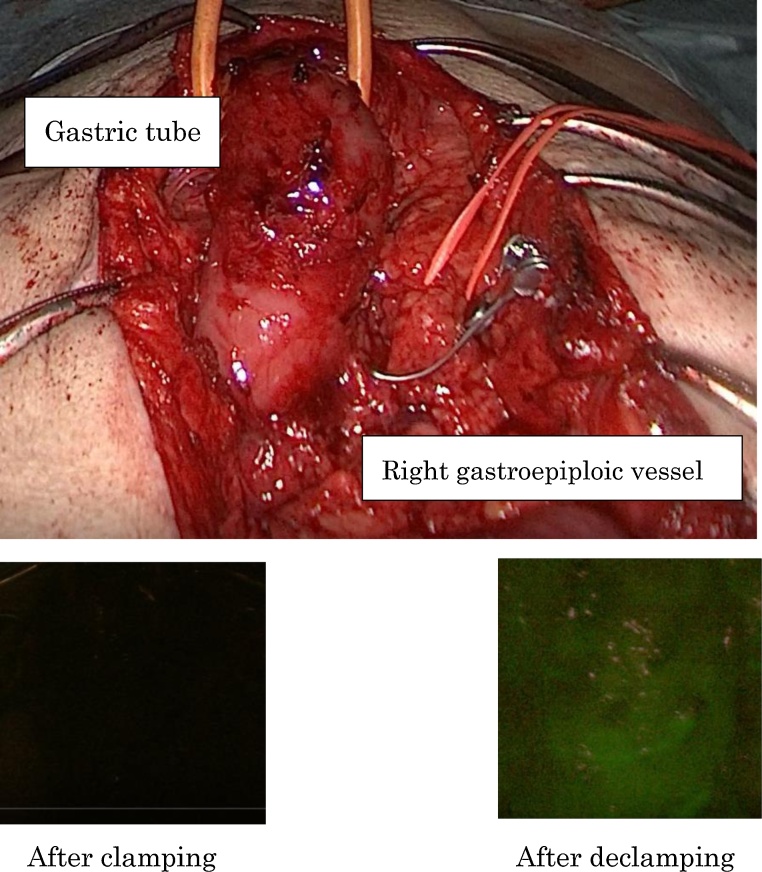
An 83-year-old man underwent subtotal esophagectomy with gastric tube reconstruction via the retrosternal route for esophageal cancer and right hemicolectomy for ascending colon cancer 16 years earlier. Postoperatively, the proximal part of the gastric tube had poor blood flow. Therefore, the patient underwent proximal-side resection of the gastric tube. Thereafter, free jejunal graft reconstruction was performed. The patient had not developed recurrence at that point. Recently, the patient visited the hospital complaining of nausea and chest discomfort. Upper gastrointestinal endoscopy revealed a type 0-IIa + IIc lesion located around the pylorus. A biopsy showed adenocarcinoma. Based on these findings, the patient was diagnosed with gastric tube cancer (cT1bN0M0StageI). The invasion depth of the cancer was predicted to be widespread submucosal invasion. Therefore, the patient underwent surgery. Intraoperatively, we evaluated the flow of the gastric tube after clamping the right gastroepiploic artery using ICG fluorescence. As a result, the flow of the gastric tube was deemed insufficient. Consequently, subtotal gastrectomy was performed with preservation of the right gastroepiploic artery via Roux-en-Y reconstruction.
ICG fluorescence is useful for evaluating the flow of the gastric tube helping to decide the operating method.
We herein report a case of subtotal gastrectomy for GTC using intraoperative ICG fluorescence.
目前,使用吲哚菁绿(ICG)荧光评估重建胃管血流的频率不断增加。然而,对于胃管癌(GTC)患者,手术方法的选择一直很困难。在此,我们报告一例ICG在GTC切除患者中有效的病例。
一名83岁男性16年前因食管癌接受了经胸骨后途径的食管次全切除术及胃管重建术,因升结肠癌接受了右半结肠切除术。术后,胃管近端血流不佳。因此,患者接受了胃管近端切除术。此后,进行了游离空肠移植重建。当时患者未出现复发。最近,患者因恶心和胸部不适前来就诊。上消化道内镜检查发现幽门周围有0-IIa + IIc型病变。活检显示为腺癌。基于这些发现,患者被诊断为胃管癌(cT1bN0M0,I期)。预计癌症浸润深度为广泛的黏膜下浸润。因此,患者接受了手术。术中,我们使用ICG荧光在夹闭胃网膜右动脉后评估胃管血流。结果,认为胃管血流不足。因此,通过Roux-en-Y重建术保留胃网膜右动脉进行了胃次全切除术。
ICG荧光有助于评估胃管血流,从而有助于决定手术方法。
我们在此报告一例使用术中ICG荧光进行GTC胃次全切除术的病例。