Escande Alexandre, Khettab Mohamed, Bockel Sophie, Dumas Isabelle, Schernberg Antoine, Gouy Sebastien, Morice Philippe, Pautier Patricia, Deutsch Eric, Haie-Meder Christine, Chargari Cyrus
Brachytherapy Unit, Gustave Roussy Cancer Campus, F-94800 Villejuif, France.
Radiotherapy Department, Gustave Roussy, F-94800 Villejuif, France.
J Clin Med. 2020 Jun 1;9(6):1653. doi: 10.3390/jcm9061653.
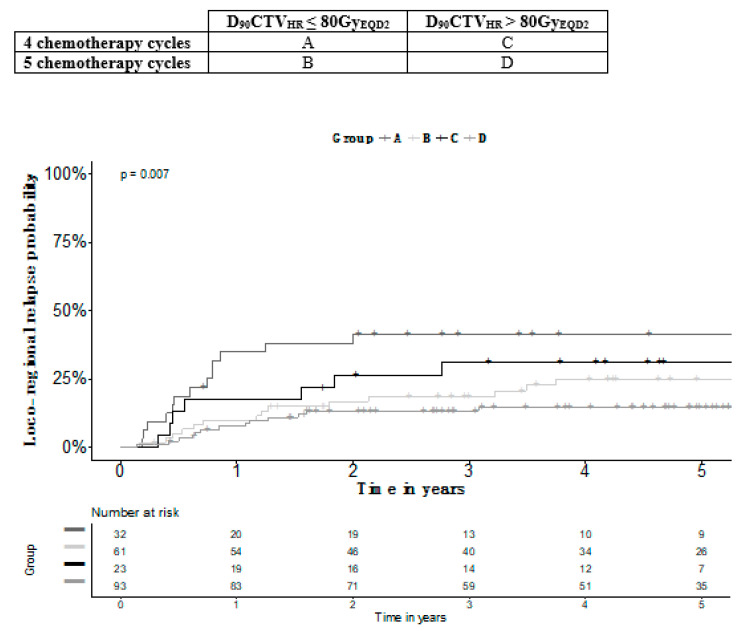
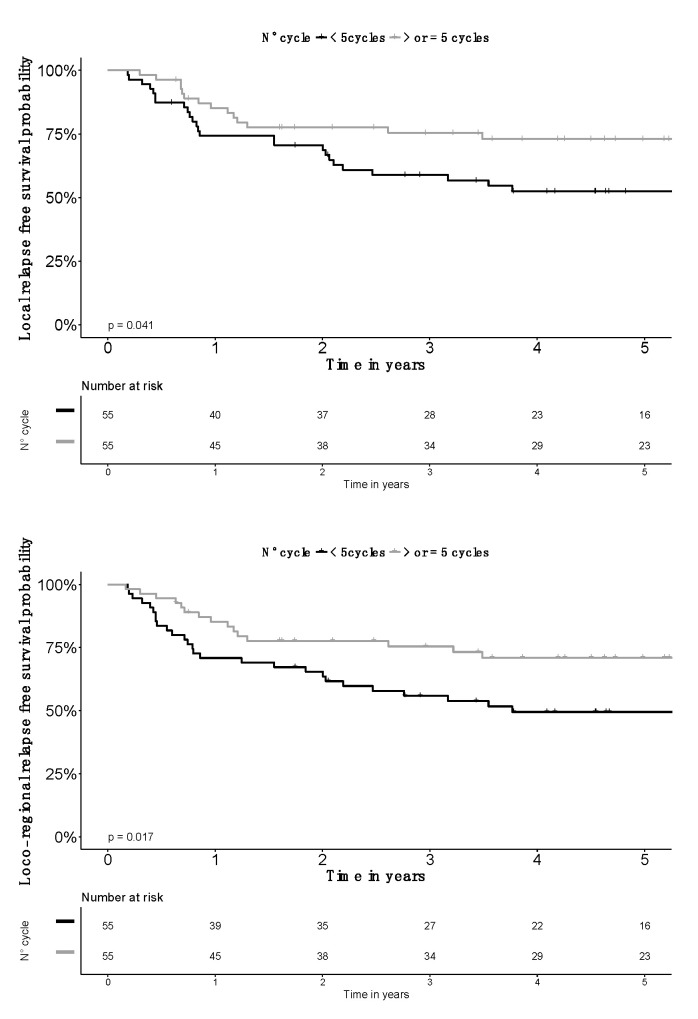
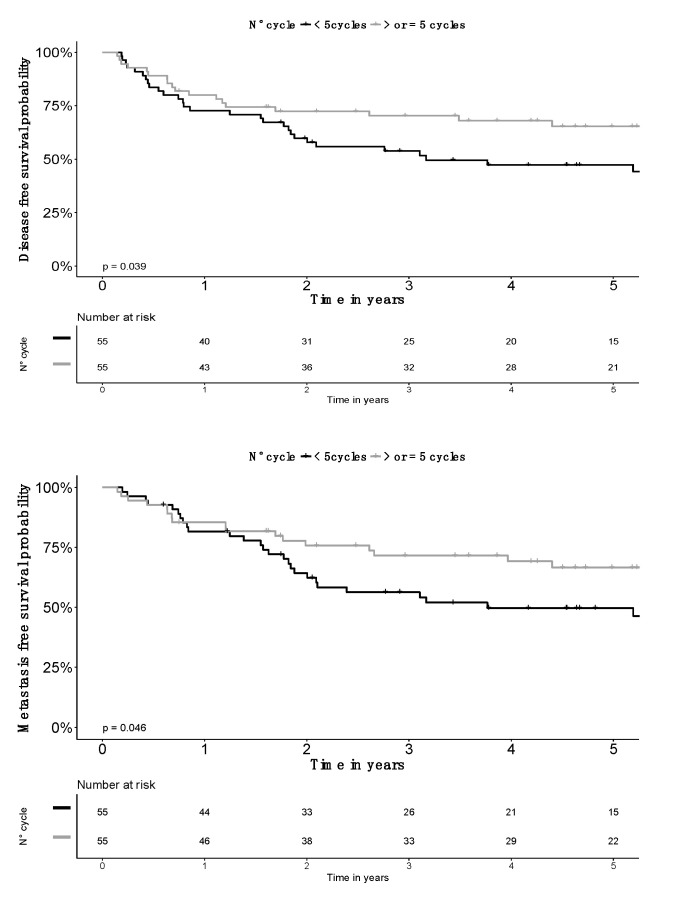
Scarce data exist on concurrent chemotherapy in locally advanced cervical cancer (LACC) patients (pts) treated with image-guided adaptive brachytherapy (IGABT). We examined the effect of a number of chemotherapy cycles and their interaction with brachytherapy dose/volume parameters. Clinical records of 209 consecutive pts treated for a LACC were reviewed. Pts received CRT concurrently with cisplatin 40 mg/m² or carboplatin AUC2. An additional cycle could have been delivered during the pulse-dose rate (PDR)-IGABT. The impact of a number of chemotherapy cycles on outcome was examined, as well as the interactions with dose volume parameters. The number of cycles was four in 55 (26.3%) pts, five in 154 (73.7%) including 101 receiving the fifth cycle during IGABT. Median follow-up was 5.5 years. Pts receiving five cycles had a better outcome on all survival endpoints, including three year local control rate (93.9% vs. 77.2%; < 0.05). In the subgroup, only pts with tumor FIGO (Fédération Internationale de Gynécologie Obstétrique) stage ≤IIB or with CTV > 25 cm had a better outcome. Pts receiving four cycles with DCTV > 80Gy had the same locoregional control-(LRC) as those receiving five cycles and achieving DCTV ≤ 80 Gy ( = 0.75). An optimal propensity score matching the balance for the FIGO stage, CTV volume and DCTV confirmed the effect, with the largest life expectancy benefit for locoregional failure-free survival (absolute gain: 1.5 years; = 0.017). Long-term radiation-induced toxicity was not increased. Increasing the total number of cycles from 4 to 5 improved LFS, suggesting a place for systemic strategies aimed at in-field cooperation. Delivering an additional cycle at the time of brachytherapy did not increase morbidity and there permitted an increase in chemotherapy dose intensity.
关于接受图像引导自适应近距离放射治疗(IGABT)的局部晚期宫颈癌(LACC)患者同时进行化疗的数据稀缺。我们研究了多个化疗周期的效果及其与近距离放射治疗剂量/体积参数的相互作用。回顾了209例连续接受LACC治疗患者的临床记录。患者接受同步放化疗,顺铂剂量为40mg/m²或卡铂AUC2。在脉冲剂量率(PDR)-IGABT期间可额外增加一个周期。研究了多个化疗周期对预后的影响以及与剂量体积参数的相互作用。55例(26.3%)患者化疗周期为4个,154例(73.7%)患者化疗周期为5个,其中101例在IGABT期间接受第5个周期。中位随访时间为5.5年。接受5个周期化疗的患者在所有生存终点方面预后更好,包括三年局部控制率(93.9%对77.2%;P<0.05)。在亚组中,仅国际妇产科联盟(FIGO)肿瘤分期≤IIB或临床靶体积(CTV)>25cm³的患者预后较好。接受4个周期且剂量计算CTV(DCTV)>80Gy的患者与接受5个周期且DCTV≤80Gy的患者局部区域控制(LRC)相同(P=0.75)。通过最佳倾向评分匹配FIGO分期、CTV体积和DCTV的平衡证实了该效果,局部区域无失败生存的预期寿命获益最大(绝对获益:1.5年;P=0.)。长期放射性毒性未增加。将化疗周期总数从4个增加到5个可改善无进展生存期(LFS),这表明旨在进行场内协作的全身治疗策略具有一定地位。在近距离放射治疗时增加一个周期不会增加发病率,且可提高化疗剂量强度。