Li Gui-You, Tan Hai-Long, Chen Pei, Hu Hui-Yu, Liu Mian, Ou-Yang Deng-Jie, Khushbu Rooh-Afza, Pun Deepak, Li Jin-Dong, Zhang Zhi-Peng, Yang Qiong, Huang Peng, Chang Shi
Department of General Surgery, Xiangya Hospital, Central South University, Changsha, Hunan, People's Republic of China.
Department of Geriatrics, Xiangya Hospital, Central South University, Changsha, Hunan, People's Republic of China.
Cancer Manag Res. 2020 May 13;12:3371-3378. doi: 10.2147/CMAR.S247914. eCollection 2020.
Therapeutic lateral neck dissection (LND) is recommended in papillary thyroid carcinoma (PTC) patients with clinically lateral lymph node metastasis (LLNM), whether underwent level V LND remains controversial for lacking of sensitive predicting system. mutation is associated with aggressive tumor behavior, recurrence, and disease-specific mortality of PTC. However, the relationship between mutation and level V LNM is unclear.
Univariate and multivariate analyses were retrospectively conducted on the potential predictive factors of 252 PTC patients who underwent initial treatment of neck lymph node dissection from September 2015 to October 2018 in our institute. mutation and the clinicopathological characteristics of the two groups were compared.
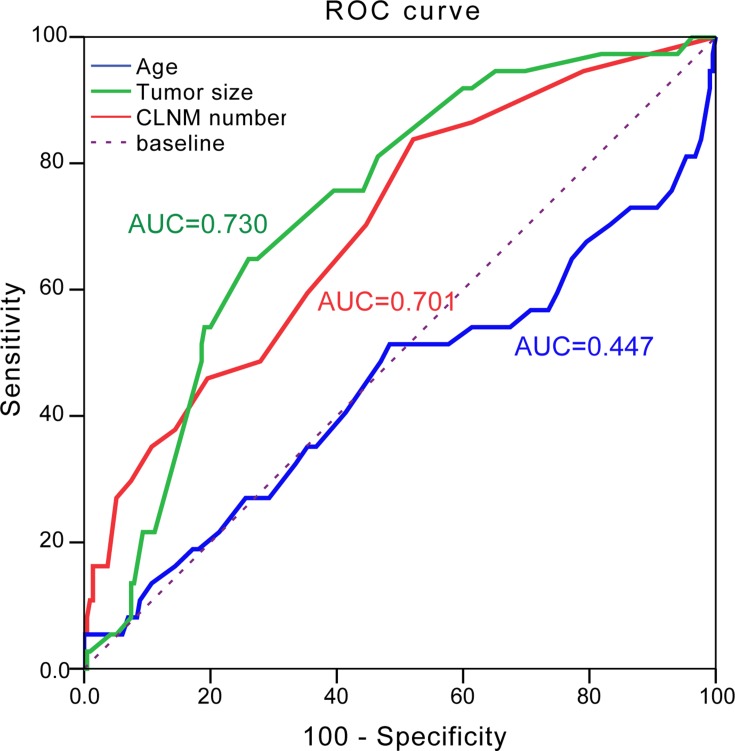
LLNM was presented in 208 (82.5%) patients and level II-V LNM was present in 42.8%, 71.2%, 85.1%, 17.8% patients, respectively. mutation was observed in 188 (74.6%) patients and was significantly associated with patients' age, lymphocytic thyroiditis, capsule invasion, bilateral central lymph node metastasis (CLNM) and level V LNM in PTC. Univariate analysis revealed that lymphocytic thyroiditis, tumor size, number of CLNM, Level II LNM, Level III LNM, simultaneous Level II+III, simultaneous Level III+IV and simultaneous Level II+III+IV were significantly correlated with Level V LNM. In addition, multivariate analysis revealed that tumor size ≥2.5 cm, number of CLNM≥3, level II metastases and mutation were independent Level V LNM predictors (odds ratio 3.910, 3.660, 8.410, 0.439; 95% CI 1.737-10.135, 1.054-12.713, 1.233-57.355, 0.280-0.827, respectively).
In summary, we presented several independent predictive factors for level V LNM in PTC patients. We constructed a risk prediction model consisting of tumor size ≥2.5 cm, number of CLNM≥3 and level II metastases and mutation that may guide surgeons to evaluate the nodal status in PTC and perform tailored therapeutic LND.
对于临床存在侧方淋巴结转移(LLNM)的甲状腺乳头状癌(PTC)患者,推荐进行治疗性侧颈淋巴结清扫术(LND),但由于缺乏敏感的预测系统,是否进行Ⅴ区LND仍存在争议。 突变与PTC的侵袭性肿瘤行为、复发及疾病特异性死亡率相关。然而, 突变与Ⅴ区LNM之间的关系尚不清楚。
回顾性分析2015年9月至2018年10月在我院接受颈部淋巴结清扫初始治疗的252例PTC患者的潜在预测因素,比较两组患者的 突变情况及临床病理特征。
208例(82.5%)患者存在LLNM,Ⅱ-Ⅴ区LNM的患者分别占42.8%、71.2%、85.1%、17.8%。188例(74.6%)患者检测到 突变,其与PTC患者的年龄、淋巴细胞性甲状腺炎、包膜侵犯、双侧中央区淋巴结转移(CLNM)及Ⅴ区LNM显著相关。单因素分析显示,淋巴细胞性甲状腺炎、肿瘤大小、CLNM数量、Ⅱ区LNM、Ⅲ区LNM、Ⅱ+Ⅲ区同时转移、Ⅲ+Ⅳ区同时转移及Ⅱ+Ⅲ+Ⅳ区同时转移与Ⅴ区LNM显著相关。此外,多因素分析显示,肿瘤大小≥2.5 cm、CLNM数量≥3、Ⅱ区转移及 突变是Ⅴ区LNM的独立预测因素(比值比分别为3.910、3.660、8.410、0.439;95%可信区间分别为1.737-10.135、1.054-12.713、1.233-57.355、0.280-0.827)。
总之,我们提出了PTC患者Ⅴ区LNM的几个独立预测因素。我们构建了一个风险预测模型,包括肿瘤大小≥2.5 cm、CLNM数量≥3、Ⅱ区转移及 突变,这可能有助于外科医生评估PTC患者的淋巴结状态并进行个体化的治疗性LND。