Siddiqui Safia, DeRemer Christina E, Waller Jennifer L, Gujral Jaspal S
Department of Medicine, Augusta University, Augusta, GA, USA.
College of Pharmacy, University of Florida, Gainesville, FL, USA.
J Innov Card Rhythm Manag. 2018 Dec 15;9(12):3428-3434. doi: 10.19102/icrm.2018.091203. eCollection 2018 Dec.
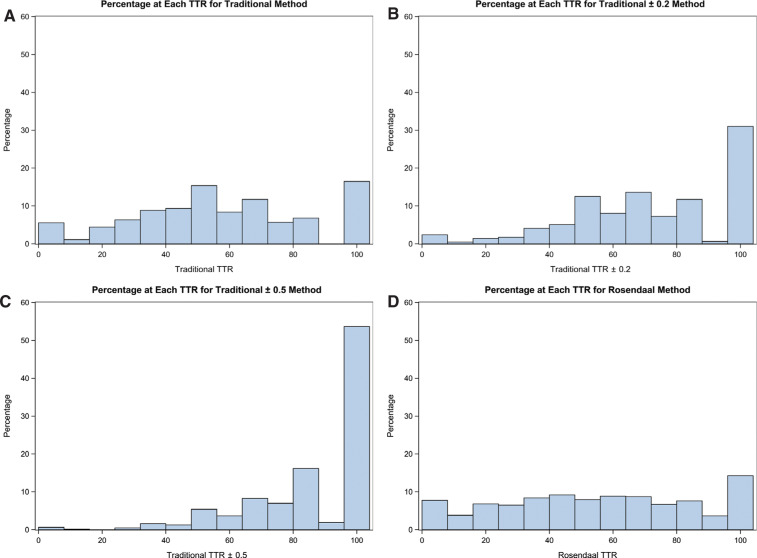
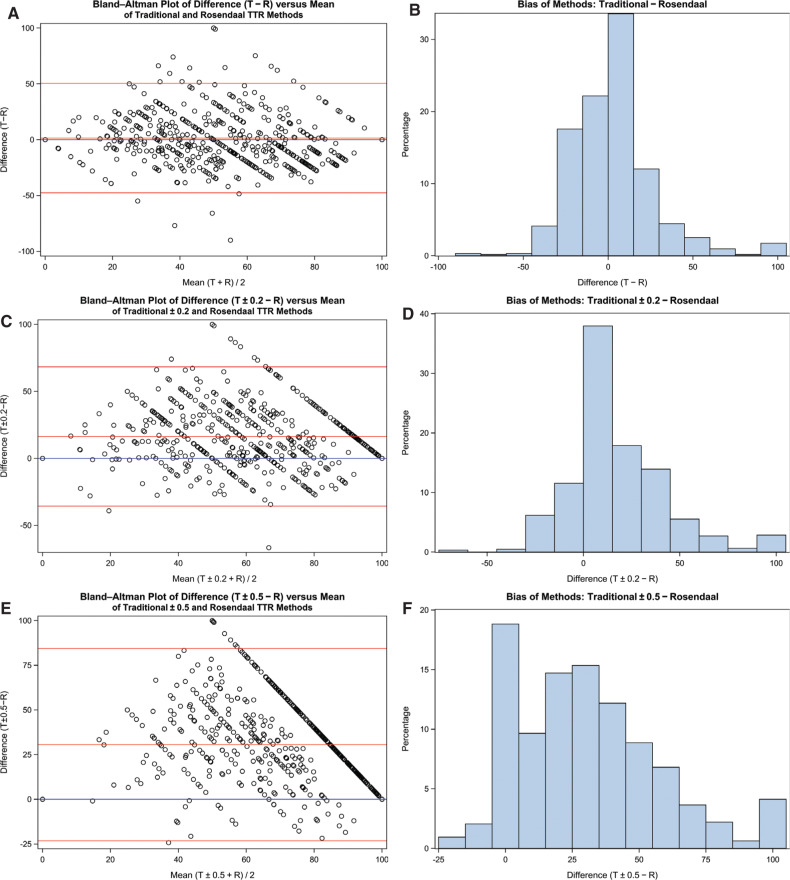
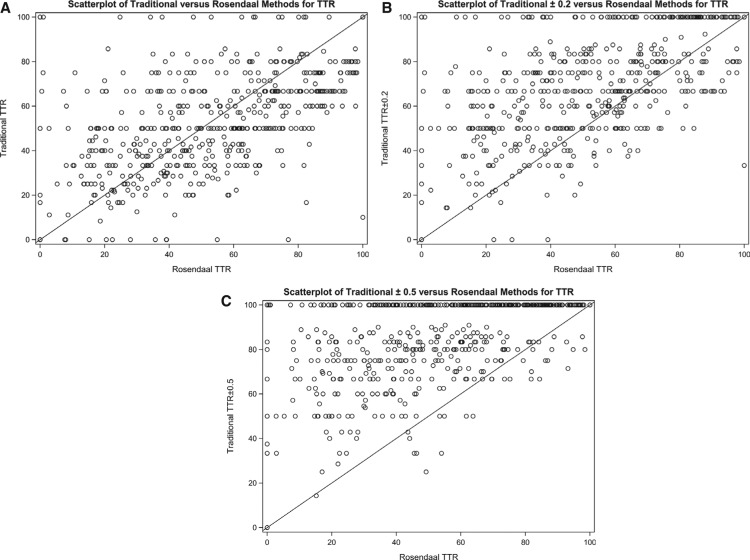
Time in therapeutic range (TTR), a well-recognized performance metric of oral anticoagulation, measures the time when patients' international normalized ratios (INRs) are within the desired range. The TTR value can vary significantly depending on the type of method used and can be a skewed indicator of the overall quality of anticoagulation. As such, the present study was designed to compare three methods for TTR calculation (cross-sectional, traditional, and Rosendaal) to quantify their differences, biases, and trends. As part of this investigation, a 21-week retrospective analysis of patients on warfarin was conducted to compare TTR values obtained by these three methods. Paired t-tests, correlation studies between size and bias, and Bland-Altman plots were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). It was revealed that the TTR values for the cross-sectional, Rosendaal, and traditional methods were 65.97, 58.12, and 51.55, respectively. The addition of tolerances to INR ranges of ± 0.2 and ± 0.5 increased TTR values to 81.79 and 91.53, respectively, for the cross-sectional method, and 66.86 and 82.69, respectively, for the traditional method. The use of the traditional method resulted in significantly higher TTR values than did use of the Rosendaal method, with high variability between the methods in both positive and negative directions. There was a demonstrated lack of independence between the methods, and zero bias could not be assumed. In conclusion, the different methods considered in the present study do not accurately measure whether a patient is in or out of the therapeutic range, and the addition of tolerances can further distort the perception of anticoagulation achieved. We recommend a standardized TTR calculation method as well as a uniform tolerance for use in clinical trials and quality control efforts.
治疗范围内时间(TTR)是口服抗凝治疗中一个广为人知的性能指标,用于衡量患者国际标准化比值(INR)处于理想范围内的时间。TTR值会因所使用方法的类型而有显著差异,并且可能是抗凝总体质量的一个有偏差的指标。因此,本研究旨在比较三种TTR计算方法(横断面法、传统法和罗森达尔法),以量化它们之间的差异、偏差和趋势。作为这项调查的一部分,对服用华法林的患者进行了为期21周的回顾性分析,以比较这三种方法获得的TTR值。使用SAS 9.4(美国北卡罗来纳州卡里市SAS研究所)进行配对t检验、大小与偏差之间的相关性研究以及布兰德-奥特曼图分析。结果显示,横断面法、罗森达尔法和传统法的TTR值分别为65.97、58.12和51.55。将INR范围的±0.2和±0.5容差加入后,横断面法的TTR值分别增至81.79和91.53,传统法的TTR值分别增至66.86和82.69。使用传统法得出的TTR值显著高于使用罗森达尔法得出的TTR值,两种方法在正负方向上都存在很大差异。已证明这些方法之间缺乏独立性,不能假定偏差为零。总之,本研究中考虑的不同方法无法准确衡量患者是否处于治疗范围内,加入容差会进一步扭曲对抗凝效果的认知。我们建议在临床试验和质量控制工作中使用标准化的TTR计算方法以及统一的容差。