Kong Feng-Wei, Wang Wei-Min, Liu Lei, Wu Wen-Bin, Wang Xiang, Zhang Miao
Department of General Surgery, Xuzhou Infectious Disease Hospital.
Department of Gastroenterology, Yichang Central People's Hospital, Institute of Digestive Disease, China Three Gorges University, Yichang.
Medicine (Baltimore). 2020 Jun 5;99(23):e20667. doi: 10.1097/MD.0000000000020667.
Pulmonary sarcomatoid carcinoma (PSC) is an uncommon type of non-small cell lung cancer, exhibiting aggressive behavior and resistance to the conventional chemoradiotherapy. To date, the optimal treatment for PSC has not been elucidated.
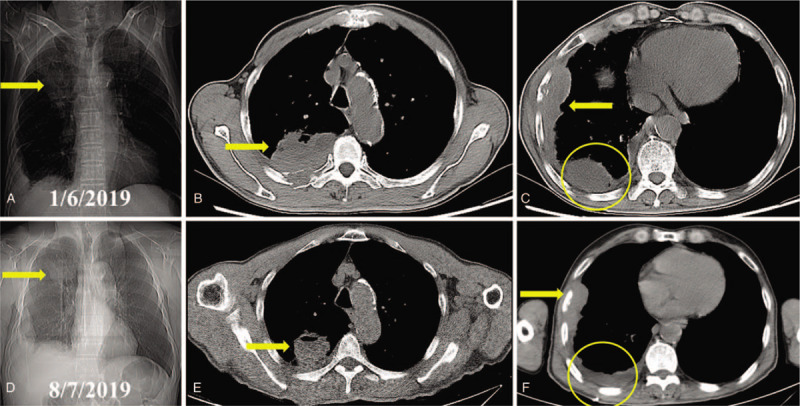
Three male patients including a 69-year-old smoker (Case 1), a 45-year-old non-smoker (Case 2), and a 69-year-old smoker (Case 3) were admitted because of cough, back pain, and loss of body weight respectively.
Radiographical examinations in these patients showed bulky intrathoracic lesions, which were pathologically diagnosed as PSC staging III-IV by computed tomography-guided percutaneous biopsy and endoscopy.
Immunotherapy was not covered by their health insurance and they refused immune checkpoint inhibitors for financial reasons. In addition, a radical resection was not appropriate due to the advanced staging of these lesions. Therefore, first-line albumin-bound paclitaxel (nab-paclitaxel, 260 mg/m of the body surface area) and carboplatin (area under curve 5) combined with oral apatinib (425 mg, daily) were administered empirically.
Two patients achieved a partial response and the other case showed stable disease lasting for more than 6 months. However, 1 of them indicated progression on the 7-month follow up.
Nab-paclitaxel/carboplatin plus apatinib showed limited short-term efficacy in advanced, unresectable PSC. The rapid resistance of PSC to the current therapeutic regimen necessitates further researches, as more effective agents are urgently needed.
肺肉瘤样癌(PSC)是一种罕见的非小细胞肺癌,具有侵袭性,且对传统放化疗耐药。迄今为止,PSC的最佳治疗方案尚未明确。
三名男性患者入院,分别为一名69岁吸烟者(病例1)、一名45岁非吸烟者(病例2)和一名69岁吸烟者(病例3),他们分别因咳嗽、背痛和体重减轻入院。
这些患者的影像学检查显示胸腔内有巨大病变,经计算机断层扫描引导下经皮活检和内镜检查,病理诊断为III-IV期PSC。
他们的医疗保险不涵盖免疫治疗,且因经济原因拒绝使用免疫检查点抑制剂。此外,由于这些病变分期较晚,根治性切除并不合适。因此,经验性给予一线白蛋白结合型紫杉醇(纳米紫杉醇,260mg/m²体表面积)和卡铂(曲线下面积5)联合口服阿帕替尼(425mg,每日)。
两名患者获得部分缓解,另一例病情稳定持续超过6个月。然而,其中1例在7个月随访时出现病情进展。
纳米紫杉醇/卡铂联合阿帕替尼在晚期、不可切除的PSC中显示出有限的短期疗效。PSC对当前治疗方案的快速耐药性需要进一步研究,因为迫切需要更有效的药物。