From the Department of Neurology (M.F., H.Y., J.C., P. Zheng., C. Zhang, F.-D.S.), Tianjin Medical University General Hospital; China National Clinical Research Center for Neurological Diseases (X. Zhang, F.-D-.S.), Jing-Jin Center for Neuroinfalmmation Beijing Tiantan Hospital, Capital Medical University; Department of Neurology (W.Q.), the Third Affiliated Hospital of Sun Yat-sen University, Guangzhou; Department of Neurology (B.B.), Tongji Hospital Affiliated to Tongji Medical College, Huazhong University of Science and Technology, Wuhan; Department of Neurology (Y.X.), Peking Union Medical College Hospital, Beijing; Xiangya Hospital of Central South University (H. Yang), Changsha; Department of Neurology (D. Huang), General Hospital of Chinese People's Liberation Army, Beijing; Division of Neurology (A.Y.L.), Department of Medicine and Therapeutics, Prince of Wales Hospital, the Chinese University of Hong Kong; Department of Neurology (J.G.), Tangdu Hospital, Air Force Military Medical University, Xi'an; Department of Neurology (M. Zhang), the First Affiliated Hospital of Shanxi Medical University, Taiyuan, China.
Neurol Neuroimmunol Neuroinflamm. 2020 Jun 4;7(5). doi: 10.1212/NXI.0000000000000787. Print 2020 Sep.
Disease-modifying drugs (DMDs) may alter the immune status and thus increase the susceptibility to coronavirus disease 2019 (COVID-19) in patients with MS or neuromyelitis optica spectrum disorders (NMOSD). However, evidence supporting this notion is currently lacking. In this study, we conducted a survey on the risk of COVID-19 in patients with MS and NMOSD.
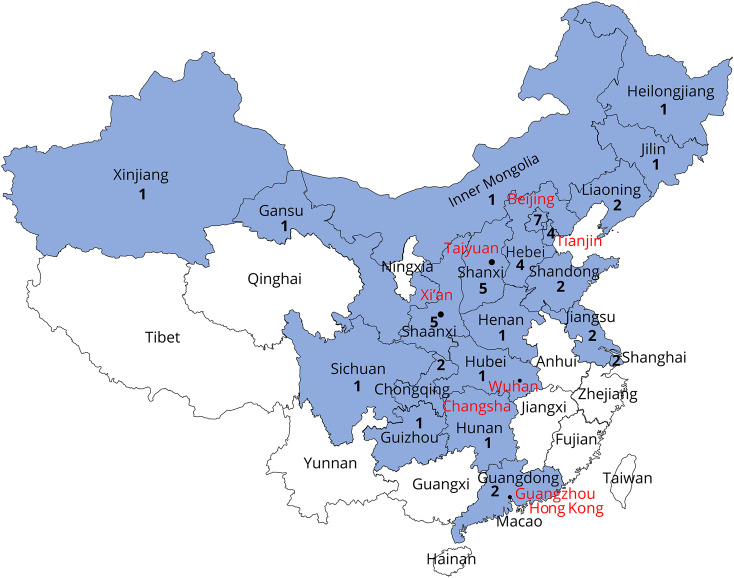
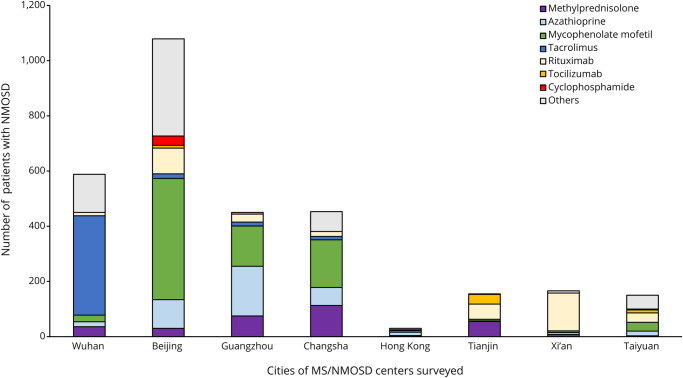
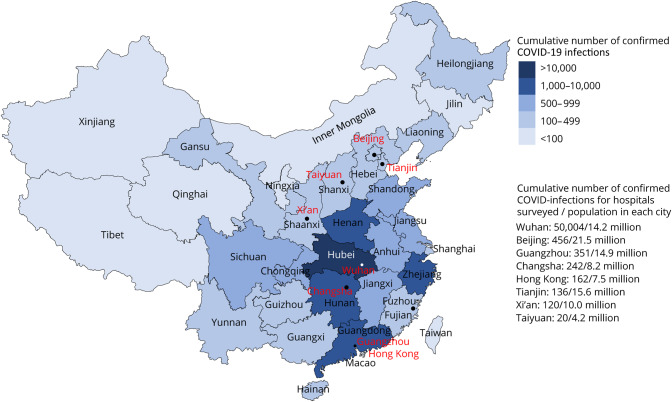
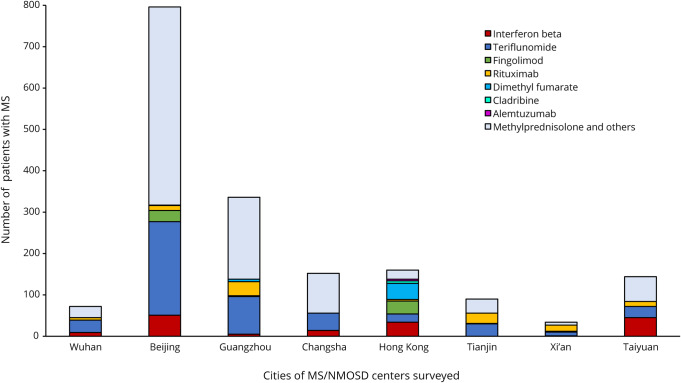
The survey was conducted through the Chinese Medical Network for Neuroinflammation. Patients in 10 MS centers from 8 cities including Wuhan were included. Information about MS and NMOSD disease duration and the usage of DMDs were collected. Data of suspected cases of COVID-19 were obtained from hospital visits, questionnaires, and patient self-reporting. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection was confirmed through clinical evaluation by a panel of experts in conjunction with chest CT and viral RNA detection.
Eight hundred eighty-two of 1,804 (48.89%) patients with MS and 2,129 of 3,060 (69.58%) patients with NMOSD were receiving DMDs. There were no alterations in the patients' DMD regimen during January 15, 2020, to March 15, 2020, the 3-month period. None of the patients with MS treated with DMDs had COVID-19. However, 2 patients with relapsing NMOSD were diagnosed with COVID-19-related pneumonia. After treatment, both patients recovered from pneumonia and neither patient experienced new attacks due to predisposing SARS-CoV-2 infection in the following 2 months.
No increased risk of COVID-19 infection was observed in patients with MS or NMOSD, irrespective of whether these patients received DMDs. A battery of stringent preventive measures adopted by neurologists to reduce COVID-19 infection in these patients may have contributed to low risk of COVID-19 infection.
疾病修饰药物(DMD)可能会改变免疫状态,从而增加多发性硬化症或视神经脊髓炎谱系疾病(NMOSD)患者感染 2019 年冠状病毒病(COVID-19)的易感性。然而,目前缺乏支持这一观点的证据。在这项研究中,我们对多发性硬化症和 NMOSD 患者的 COVID-19 风险进行了调查。
该调查通过中国神经炎症医学网络进行。纳入了来自武汉等 8 个城市的 10 个 MS 中心的患者。收集了 MS 和 NMOSD 疾病持续时间以及 DMD 使用情况的信息。通过医院就诊、问卷调查和患者自我报告获得疑似 COVID-19 病例的数据。通过专家组的临床评估,结合胸部 CT 和病毒 RNA 检测,确认严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)感染。
882 名多发性硬化症患者(48.89%)和 2129 名 NMOSD 患者(69.58%)正在接受 DMD 治疗。2020 年 1 月 15 日至 3 月 15 日,即 3 个月期间,患者的 DMD 方案没有改变。未发现接受 DMD 治疗的多发性硬化症患者发生 COVID-19。然而,2 例复发型 NMOSD 患者被诊断为 COVID-19 相关肺炎。经治疗,2 例患者均痊愈,且在接下来的 2 个月内,均未因 SARS-CoV-2 感染而导致新的发作。
接受或未接受 DMD 治疗的多发性硬化症或 NMOSD 患者均未观察到 COVID-19 感染风险增加。神经科医生采取了一系列严格的预防措施,以降低这些患者的 COVID-19 感染风险,可能是 COVID-19 感染风险较低的原因。