College of Medicine and Public Health, Flinders University, Adelaide, South Australia, Australia
College of Medicine and Public Health, Flinders University, Adelaide, South Australia, Australia.
J Immunother Cancer. 2020 Jun;8(1). doi: 10.1136/jitc-2019-000500.
Preliminary evidence indicates that early tumor shrinkage (ETS) following immune checkpoint inhibitor (ICI) initiation may be associated with survival outcomes in patients with advanced melanoma. ETS has not been explored as a biomarker of survival outcomes or patient-reported outcomes in patients with advanced non-small cell lung cancer (NSCLC) treated with ICIs.
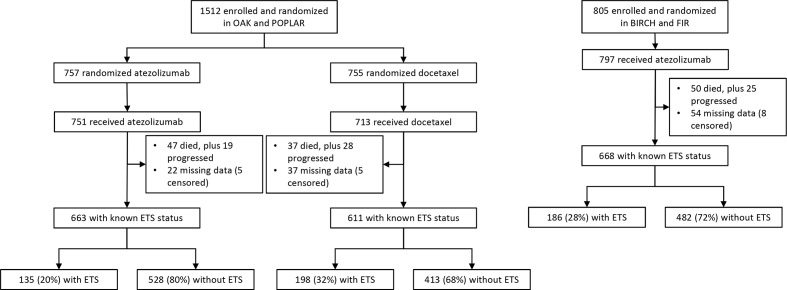
The study pooled data from patients with NSCLC in the randomized trials OAK and POPLAR (atezolizumab vs docetaxel; n=1464), and single-arm atezolizumab trials BIRCH and FIR (n=797). The association between ETS (≥10% decrease in pretreatment sum-of-longest diameters of target-lesions at 6 weeks) and overall survival (OS), progression-free survival (PFS), time to deterioration (TDD) in health-related quality-of-life (HRQoL) and physical function (PF) was assessed using Cox proportional hazard analysis.
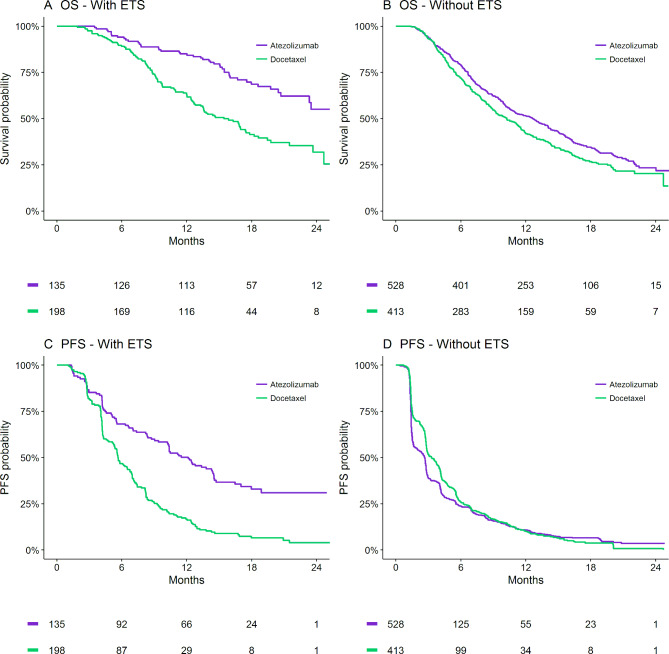
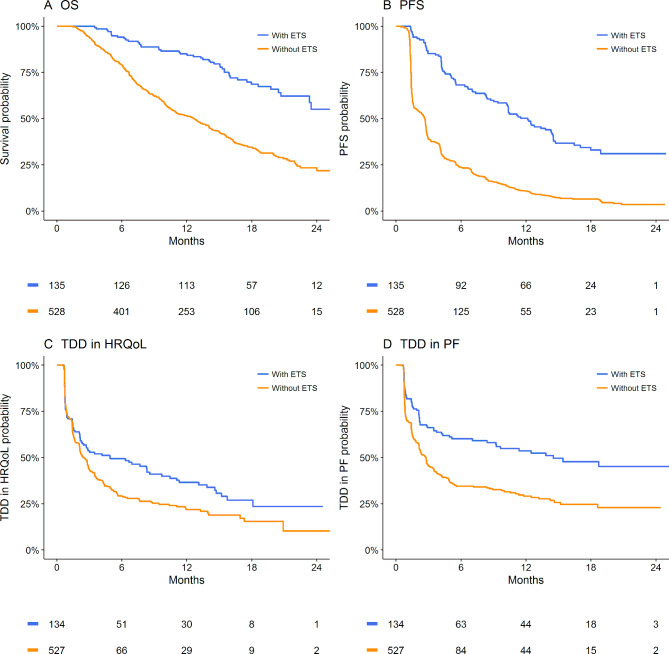
ETS occurred in 20% of atezolizumab-treated patients with NSCLC within OAK and POPLAR and was associated with highly favorable OS (HR 0.33, p<0.001), PFS (HR 0.31, p<0.001), TDD in HRQoL (HR 0.73, p=0.01) and PF (HR 0.52, p<0.001). The results were replicated in the BIRCH and FIR data. Atezolizumab-treated patients achieving ETS had markedly improved OS compared with docetaxel-treated patients achieving ETS (24-month OS 55% vs 32%); PFS was also markedly improved (24-month PFS 31% vs 4%). In contrast, for patients not achieving ETS, atezolizumab-treatment was associated with more modest OS (24-month OS 23% vs 20%) and PFS (24-month PFS 3% vs 1%) improvement compared with docetaxel. Overall, the effect size for ETS within the atezolizumab-treated patients was significantly greater than that in the docetaxel-treated patients (P(interaction)=0.002 for OS and P(interaction)<0.001 for PFS).
ETS is an easily measurable biomarker, predictive of highly favorable survival and patient-reported outcomes with atezolizumab treatment for advanced NSCLC. Further, ETS identifies patients with significantly greater treatment benefit for ICI therapy.
初步证据表明,免疫检查点抑制剂(ICI)治疗后早期肿瘤缩小(ETS)可能与晚期黑色素瘤患者的生存结局相关。在接受 ICI 治疗的晚期非小细胞肺癌(NSCLC)患者中,ETS 尚未被探索作为生存结局或患者报告结局的生物标志物。
本研究汇总了来自 OAK 和 POPLAR(阿替利珠单抗对比多西他赛;n=1464)随机试验以及单臂阿替利珠单抗试验 BIRCH 和 FIR(n=797)中 NSCLC 患者的数据。使用 Cox 比例风险分析评估 ETS(治疗前最长直径总和在 6 周时下降≥10%)与总生存期(OS)、无进展生存期(PFS)、健康相关生活质量(HRQoL)和身体功能(PF)恶化时间(TDD)之间的关联。
在 OAK 和 POPLAR 中,20%接受阿替利珠单抗治疗的 NSCLC 患者发生 ETS,且 ETS 与非常有利的 OS(HR 0.33,p<0.001)、PFS(HR 0.31,p<0.001)、HRQoL 的 TDD(HR 0.73,p=0.01)和 PF(HR 0.52,p<0.001)相关。BIRCH 和 FIR 数据中的结果得到了复制。与阿替利珠单抗治疗达到 ETS 的患者相比,多西他赛治疗达到 ETS 的患者 OS 显著改善(24 个月 OS 55% vs 32%);PFS 也明显改善(24 个月 PFS 31% vs 4%)。相比之下,对于未达到 ETS 的患者,与多西他赛相比,阿替利珠单抗治疗与适度的 OS(24 个月 OS 23% vs 20%)和 PFS(24 个月 PFS 3% vs 1%)改善相关。总体而言,在阿替利珠单抗治疗患者中 ETS 的效应大小显著大于多西他赛治疗患者(OS 时 P(交互)=0.002,PFS 时 P(交互)<0.001)。
ETS 是一种易于测量的生物标志物,可预测晚期 NSCLC 患者接受阿替利珠单抗治疗的高度有利的生存和患者报告结局。此外,ETS 可识别出对 ICI 治疗具有显著更大治疗益处的患者。