Biancalana Edoardo, Parolini Federico, Mengozzi Alessandro, Solini Anna
Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy.
Department of Surgical, Medical, Molecular and Critical Area Pathology, University of Pisa, Via Roma 67, 56126 Pisa, Italy.
Diabetol Metab Syndr. 2020 May 25;12:47. doi: 10.1186/s13098-020-00555-x. eCollection 2020.
Type 2 diabetes (T2D) shows a high mortality rate, dependent on disease duration, comorbidities and glucose control over time. Data on patients with short disease duration are scanty.
We prospectively followed a cohort of newly-diagnosed T2D patients referring to a single diabetes centre, treated according to the international guidelines and checked every 6-12 months. All-cause mortality and major cardiovascular (CV) events were registered.
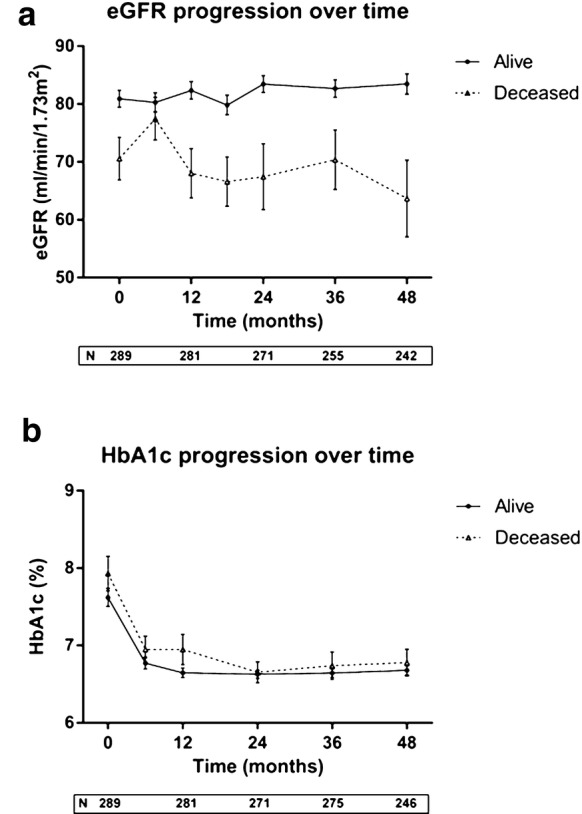
289 patients out of 3019 consecutive first attendances matched inclusion criteria and were included in the observation. Mean follow-up was 51.2 months. At 31 December 2018, 253 patients were alive and 36 deceased. At baseline, deceased individuals were older, with lower eGFR and lower uric acid, higher prevalence of atrial fibrillation. During the follow-up, 18 non-fatal CV events were adjudicated; patients with incident CV disease (CVD) differed at baseline for sex, previous history of CVD and retinopathy, higher use of secretagogues and lower use of metformin. At multivariate analysis, age and previous CVD were the only independent determinants of all-cause mortality and incident CVD, respectively. In deceased individuals, eGFR slope was markedly unstable and ΔeGFR at the end of the follow-up was higher (p < 0.001), and predicted mortality.
Newly-diagnosed T2D patients followed according to the best clinical practice show a mortality rate similar to that reported in more complicated patients with longer disease duration; none of the clinical and biochemical variables commonly measured at baseline can predict mortality or incident CVD; early metformin use seems to be associated with no risk of prevalent or incident retinopathy.
2型糖尿病(T2D)死亡率较高,这取决于疾病持续时间、合并症以及长期的血糖控制情况。关于病程较短患者的数据较少。
我们对一批新诊断的T2D患者进行了前瞻性随访,这些患者均前往单一糖尿病中心就诊,按照国际指南进行治疗,并每6 - 12个月进行检查。记录全因死亡率和主要心血管(CV)事件。
3019例连续首次就诊患者中,有289例符合纳入标准并被纳入观察。平均随访时间为51.2个月。截至2018年12月31日,253例患者存活,36例死亡。基线时,死亡患者年龄更大,估算肾小球滤过率(eGFR)和尿酸更低,房颤患病率更高。随访期间,判定发生了18例非致命性CV事件;发生心血管疾病(CVD)的患者在基线时在性别、既往CVD和视网膜病变史、促泌剂使用较多以及二甲双胍使用较少方面存在差异。多变量分析显示,年龄和既往CVD分别是全因死亡率和新发CVD的唯一独立决定因素。在死亡患者中,eGFR斜率明显不稳定,随访结束时的ΔeGFR更高(p < 0.001),且可预测死亡率。
按照最佳临床实践进行随访的新诊断T2D患者的死亡率与报道的病程较长的更复杂患者相似;基线时常规测量的临床和生化变量均无法预测死亡率或新发CVD;早期使用二甲双胍似乎与发生或患视网膜病变的风险无关。