Appelboam Andrew, Green Jonathan, Ewings Paul, Black Sarah
University of Exeter Medical School, St Luke's, Exeter, Devon UK.
Academic Department of Emergency Medicine, Royal Devon and Exeter Hospital NHS Foundation Trust, Exeter, Devon UK.
Pilot Feasibility Stud. 2020 May 25;6:74. doi: 10.1186/s40814-020-00616-y. eCollection 2020.
The valsalva manoeuvre is an internationally recommended initial treatment for supraventricular tachycardia (SVT). The pre-hospital use of a valsalva assist device, to help deliver this manoeuvre, could improve cardioversion rates and reduce the need for patients to attend hospital.
We conducted a randomised controlled feasibility trial comparing ambulance clinician use of a valsalva assist device versus standard care to treat adult patients presenting to an ambulance service in the south west of England. Eligible consenting participants were randomised 1:1 to device or standard care with trial procedures mirroring a proposed definitive trial.Feasibility was assessed upon ambulance clinician and participant recruitment rates and feedback, data completeness and potential future primary outcome rates.
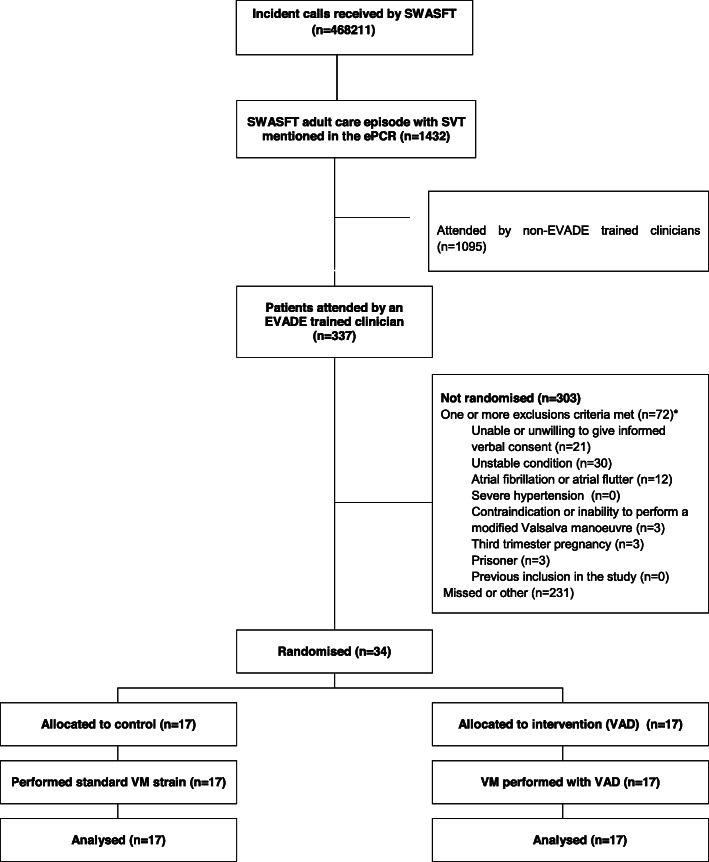
Over a 6 months period (1 July to 31 December 2018), 276 (23%) of 1183 eligible ambulance clinicians were trained and they recruited 34 participants; approximately 10% of patients presenting with suspected SVT during that time. Seventeen participants were randomised to each arm and all underwent their allocated valsalva strain method. All trial data and 63/68 (93%) of pre and post-valsalva ECGs were available. Seven (21%) participants had ineligible initial rhythms on retrospective expert ECG review. Valsalva assist device use was associated with cardioversion and non-conveyance in 4 (24%) and 2 (12%) participants respectively. No participants assigned to standard care were cardioverted and all were conveyed. Participant feedback highlighted the challenges of retaining trial information during an SVT attack.
The trial achieved efficient clinician training, randomisation and data collection, and there was an encouraging effect signal associated with device use. However, trial design changes should be considered to address the relatively small proportion of eligible patients recruited and challenges identified with consent and confirmation of cardioversion as a primary outcome.
The trial was registered with ClinicalTrials.gov (NCT03514628) on 2 May 2018.
瓦尔萨尔瓦动作是国际上推荐的室上性心动过速(SVT)初始治疗方法。院前使用瓦尔萨尔瓦辅助装置来协助实施该动作,可能会提高复律率,并减少患者前往医院就诊的需求。
我们进行了一项随机对照可行性试验,比较救护车临床医生使用瓦尔萨尔瓦辅助装置与标准治疗方法,以治疗英格兰西南部救护服务机构接收的成年患者。符合条件且同意参与的受试者被1:1随机分配至使用装置组或标准治疗组,试验程序模仿拟进行的确定性试验。根据救护车临床医生和受试者招募率及反馈、数据完整性以及潜在的未来主要结局发生率来评估可行性。
在6个月期间(2018年7月1日至12月31日),1183名符合条件的救护车临床医生中有276名(23%)接受了培训,他们招募了34名受试者;约占该时间段内疑似SVT患者的10%。每组随机分配了17名受试者,所有受试者均采用了各自分配的瓦尔萨尔瓦用力方法。所有试验数据以及68份瓦尔萨尔瓦动作前后心电图中的63份(93%)均可用。经回顾性专家心电图审查,7名(21%)受试者的初始心律不符合条件。使用瓦尔萨尔瓦辅助装置的受试者中分别有4名(24%)复律且未被送往医院,2名(12%)未被送往医院。分配至标准治疗组的受试者均未复律,全部被送往医院。受试者反馈强调了在SVT发作期间保留试验信息的挑战。
该试验实现了高效的临床医生培训、随机分组和数据收集,并且使用装置有令人鼓舞的效果信号。然而,应考虑改变试验设计,以解决招募的符合条件患者比例相对较小以及在同意和将复律确认为主要结局方面发现的挑战。
该试验于2018年5月2日在ClinicalTrials.gov(NCT03514628)注册。