Raffaelli Bianca, Kalantzis Rea, Mecklenburg Jasper, Overeem Lucas Hendrik, Neeb Lars, Gendolla Astrid, Reuter Uwe
Department of Neurology, Charité Universitätsmedizin Berlin, Berlin, Germany.
Clinician Scientist Program, Berlin Institute of Health (BIH), Berlin, Germany.
Front Neurol. 2020 May 28;11:417. doi: 10.3389/fneur.2020.00417. eCollection 2020.
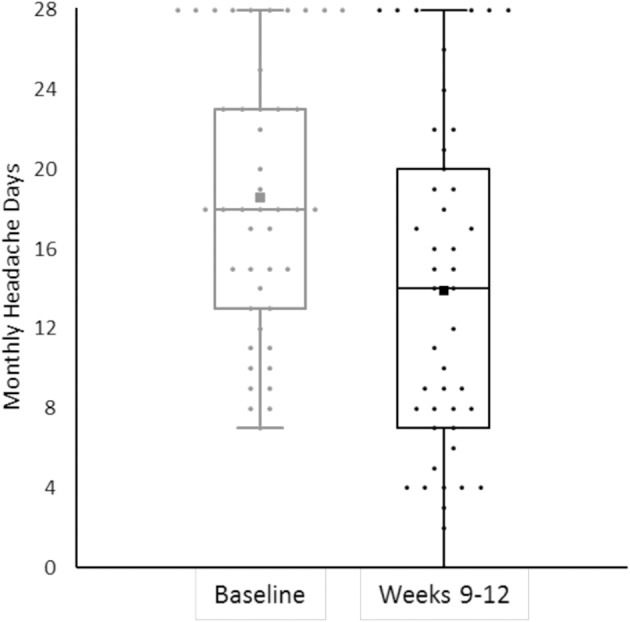
German authorities reimburse migraine prevention with erenumab only in patients who previously did not have therapeutic success with at least five oral prophylactics or have contraindications to such. In this real-world analysis, we assessed treatment response to erenumab in patients with chronic migraine (CM) who failed five oral prophylactics and, in addition, onabotulinumtoxinA (BoNTA). We analyzed retrospective data of 139 CM patients with at least one injection of erenumab from two German headache centers. Patients previously did not respond sufficiently or had contraindications to β-blockers, flunarizine, topiramate, amitriptyline, valproate, and BoNTA. Primary endpoint of this analysis was the mean change in monthly headache days from the 4-weeks baseline period over the course of a 12-weeks erenumab therapy. Secondary endpoints were changes in monthly migraine days, days with severe headache, days with acute headache medication, and triptan intake in the treatment period. Erenumab (starting dose 70 mg) led to a reduction of -3.7 (95% CI 2.4-5.1) monthly headache days after the first treatment and -4.7 (95% CI 2.9-6.5) after three treatment cycles ( < 0.001 for both). All secondary endpoint parameters were reduced over time. Half of patients (51.11%) had a >30% reduction of monthly headache days in weeks 9-12. Only 4.3% of the patients terminated erenumab treatment due to side effects. In this treatment-refractory CM population, erenumab showed efficacy in a real-world setting similar to data from clinical trials. Tolerability was good, and no safety issues emerged. Erenumabis is a treatment option for CM patients who failed all first-line preventives in addition to BoNTA.
德国当局仅对之前使用至少五种口服预防性药物治疗未取得成功或对此类药物有禁忌症的偏头痛患者报销erenumab用于预防偏头痛的费用。在这项真实世界分析中,我们评估了在口服五种预防性药物且此外还使用了A型肉毒毒素(BoNTA)均失败的慢性偏头痛(CM)患者中erenumab的治疗反应。我们分析了来自两个德国头痛中心的139例至少注射过一次erenumab的CM患者的回顾性数据。这些患者之前对β受体阻滞剂、氟桂利嗪、托吡酯、阿米替林、丙戊酸盐和BoNTA反应欠佳或有禁忌症。该分析的主要终点是在12周erenumab治疗过程中,从4周基线期开始每月头痛天数的平均变化。次要终点是治疗期内每月偏头痛天数、重度头痛天数、急性头痛药物使用天数和曲坦类药物摄入量的变化。Erenumab(起始剂量70mg)在首次治疗后使每月头痛天数减少了-3.7(95%CI 2.4-5.1),三个治疗周期后减少了-4.7(95%CI 2.9-6.5)(两者均P<0.001)。所有次要终点参数均随时间减少。半数患者(51.11%)在第9至12周每月头痛天数减少>30%。仅4.3%的患者因副作用终止erenumab治疗。在这个治疗难治性CM人群中,erenumab在真实世界环境中显示出与临床试验数据相似的疗效。耐受性良好,未出现安全性问题。对于除BoNTA外所有一线预防性药物均治疗失败的CM患者,erenumab是一种治疗选择。