Department of Women's and Children's Health, International Maternal and Child Health (IMCH), Uppsala University, Uppsala, Sweden.
Department of Parasitology and Medical Entomology, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania.
Malar J. 2020 Jun 23;19(1):216. doi: 10.1186/s12936-020-03287-5.
Artemisinin-based combination therapy (ACT) resistant Plasmodium falciparum represents an increasing threat to Africa. Extended ACT regimens from standard 3 to 6 days may represent a means to prevent its development and potential spread in Africa.
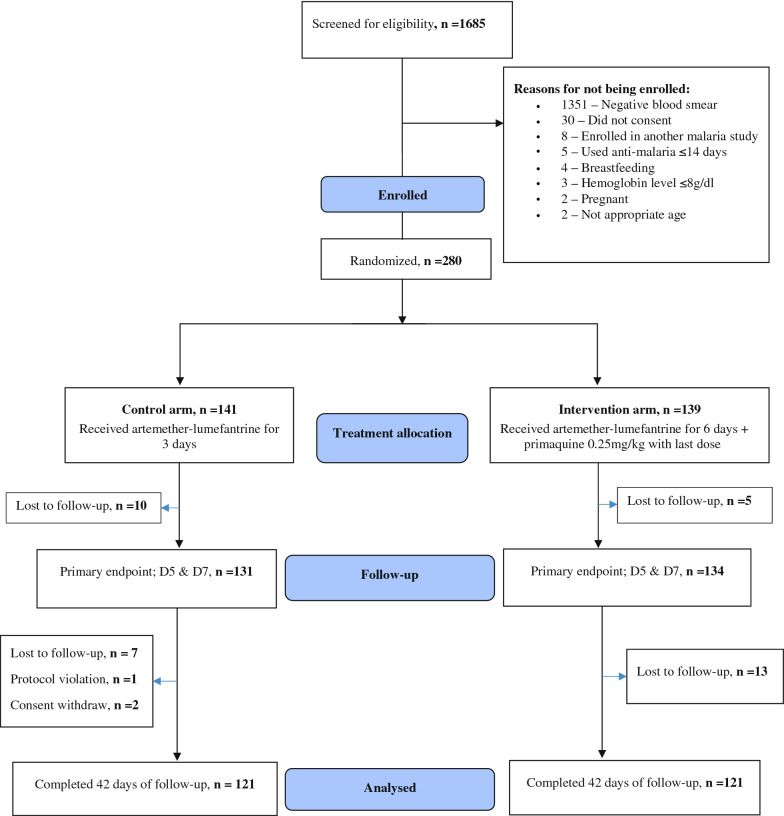
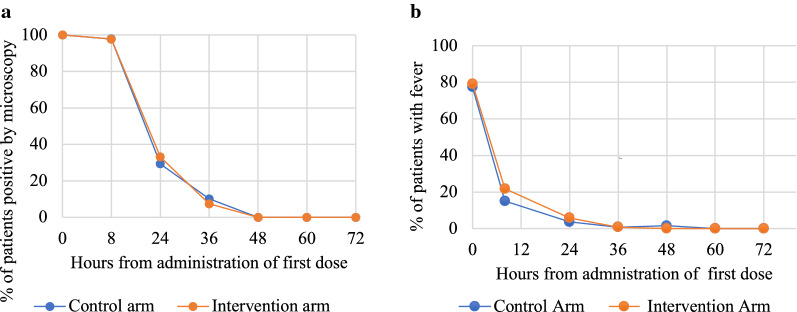
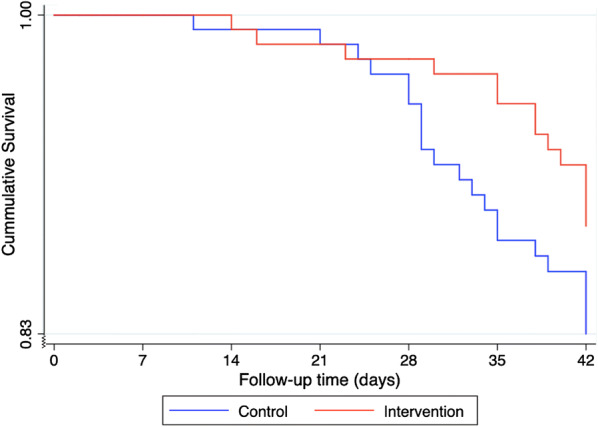
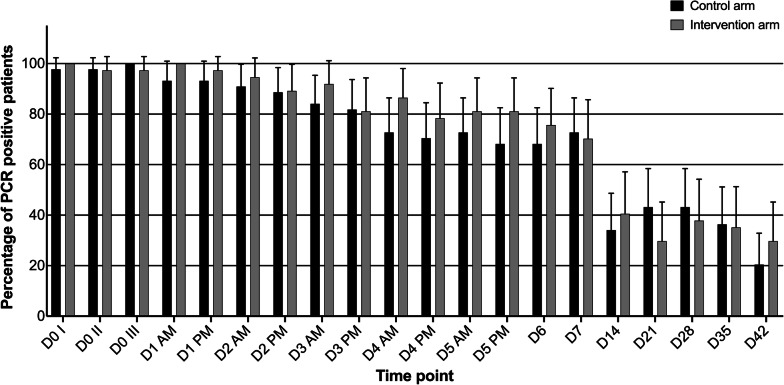
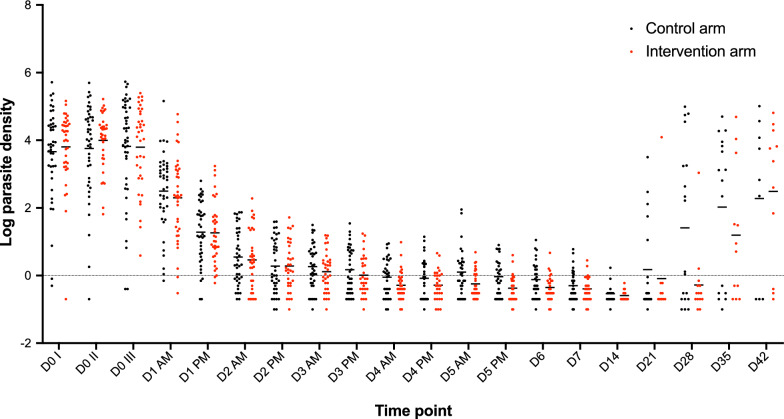
Standard 3-day treatment with artemether-lumefantrine (control) was compared to extended 6-day treatment and single low-dose primaquine (intervention); in a randomized controlled, parallel group, superiority clinical trial of patients aged 1-65 years with microscopy confirmed uncomplicated P. falciparum malaria, enrolled in Bagamoyo district, Tanzania. The study evaluated parasite clearance, including proportion of PCR detectable P. falciparum on days 5 and 7 (primary endpoint), cure rate, post-treatment prophylaxis, safety and tolerability. Clinical, and laboratory assessments, including ECG were conducted during 42 days of follow-up. Blood samples were collected for parasite detection (by microscopy and PCR), molecular genotyping and pharmacokinetic analyses. Kaplan-Meier survival analyses were done for both parasite clearance and recurrence.
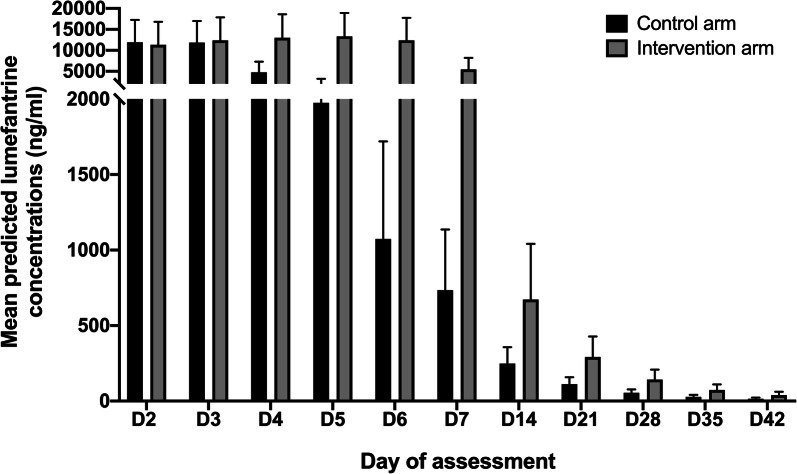
A total of 280 patients were enrolled, 141 and 139 in the control and intervention arm, respectively, of whom 121 completed 42 days follow-up in each arm. There was no difference in proportion of PCR positivity across the arms at day 5 (80/130 (61.5%) vs 89/134 (66.4%), p = 0.44), or day 7 (71/129 (55.0%) vs 70/134 (52.2%), p = 0.71). Day 42 microscopy determined cure rates (PCR adjusted) were 97.4% (100/103) and 98.3% (110/112), p = 0.65, in the control and intervention arm, respectively. Microscopy determined crude recurrent parasitaemia during follow-up was 21/121 (17.4%) in the control and 14/121 (11.6%) in the intervention arm, p = 0.20, and it took 34 days and 42 days in the respective arms for 90% of the patients to remain without recurrent parasitaemia. Lumefantrine exposure was significantly higher in intervention arm from D3 to D42, but cardiac, biochemical and haematological safety was high and similar in both arms.
Extended 6-day artemether-lumefantrine treatment and a single low-dose of primaquine was not superior to standard 3-day treatment for ACT sensitive P. falciparum infections but, importantly, equally efficacious and safe. Thus, extended artemether-lumefantrine treatment may be considered as a future treatment regimen for ACT resistant P. falciparum, to prolong the therapeutic lifespan of ACT in Africa. Trial registration ClinicalTrials.gov, NCT03241901. Registered July 27, 2017 https://clinicaltrials.gov/show/NCT03241901.
青蒿素为基础的联合疗法(ACT)耐药性恶性疟原虫对非洲构成越来越大的威胁。将标准的 3 天 ACT 疗程延长至 6 天可能是预防其在非洲发展和潜在传播的一种手段。
采用青蒿琥酯-咯萘啶(对照)标准 3 天治疗,与延长 6 天治疗和单低剂量磷酸伯氨喹(干预)进行比较;在坦桑尼亚巴加莫约区进行了一项随机对照、平行组、优势临床试验,纳入年龄在 1-65 岁之间、经显微镜证实患有单纯性恶性疟原虫疟疾的患者。该研究评估了寄生虫清除情况,包括第 5 天和第 7 天 PCR 检测到的疟原虫比例(主要终点)、治愈率、治疗后预防、安全性和耐受性。在 42 天的随访期间进行了临床和实验室评估,包括心电图检查。采集血液样本进行寄生虫检测(通过显微镜和 PCR)、分子基因分型和药代动力学分析。采用 Kaplan-Meier 生存分析方法对寄生虫清除和复发进行分析。
共纳入 280 例患者,对照组和干预组各 141 例和 139 例,每组各有 121 例患者完成了 42 天随访。第 5 天(80/130(61.5%)vs 89/134(66.4%),p=0.44)和第 7 天(71/129(55.0%)vs 70/134(52.2%),p=0.71)两组的 PCR 阳性比例无差异。第 42 天显微镜确定的治愈率(PCR 校正)分别为对照组 97.4%(100/103)和干预组 98.3%(110/112),p=0.65。对照组和干预组在随访期间出现显微镜确定的复发性寄生虫血症的粗发生率分别为 21/121(17.4%)和 14/121(11.6%),p=0.20。分别有 90%的患者在各自的治疗组中需要 34 天和 42 天才能不再出现复发性寄生虫血症。从第 3 天到第 42 天,干预组的青蒿琥酯暴露量明显高于对照组,但心脏、生化和血液学安全性均较高,两组相似。
延长 6 天的青蒿琥酯-咯萘啶治疗和单低剂量磷酸伯氨喹治疗对敏感的 ACT 恶性疟原虫感染并不优于标准的 3 天治疗,但同样有效且安全。因此,延长青蒿琥酯-咯萘啶治疗可能被考虑作为治疗 ACT 耐药性恶性疟原虫的未来治疗方案,以延长 ACT 在非洲的治疗寿命。
ClinicalTrials.gov,NCT03241901。2017 年 7 月 27 日注册https://clinicaltrials.gov/show/NCT03241901。