Gordhandas Sushmita, Kahn Ryan M, Gamble Charlotte, Talukdar Nizam, Maddy Brandon, Baltich Nelson Becky, Askin Gulce, Christos Paul J, Holcomb Kevin, Caputo Thomas A, Chapman-Davis Eloise, Frey Melissa K
Department of Obstetrics and Gynecology, Weill Cornell Medical College, New York, NY, USA.
Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, Weill Cornell Medical College, New York, NY, USA.
Ecancermedicalscience. 2020 Jun 18;14:1061. doi: 10.3332/ecancer.2020.1061. eCollection 2020.
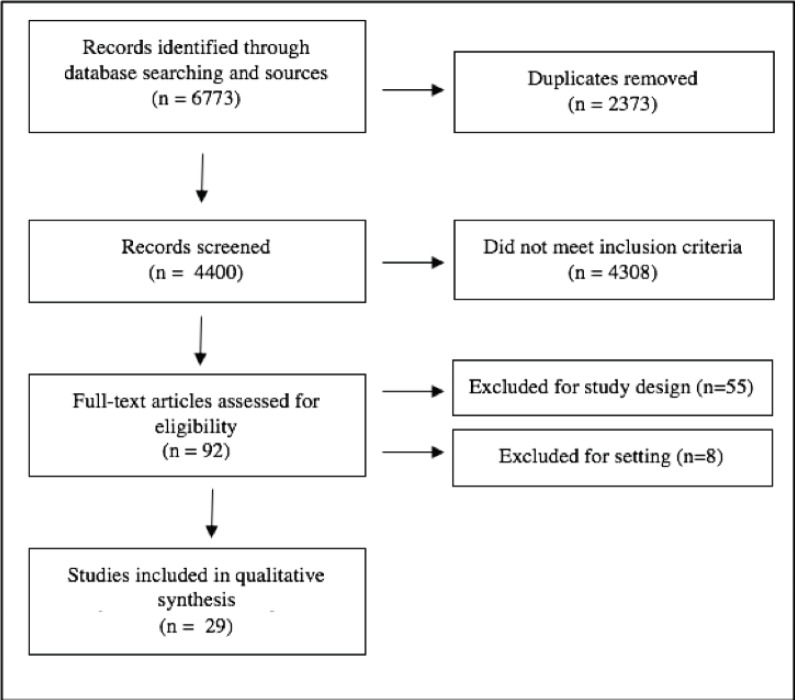
The inclusion of DNA mismatch repair (MMR) evaluation as a standard of care for endometrial cancer management will result in a growing population of patients with MMR deficiency and negative germline Lynch syndrome testing (MMR-deficient). In this systematic review and study, the clinicopathologic features of endometrial cancer in patients with MMR-intact, MLH1 methylation positive, MMR-deficient or Lynch syndrome are evaluated. A systematic search of online databases between 1990 and 2018 identified studies of endometrial cancer patients with tumour testing (MMR protein immunohistochemistry or microsatellite instability) and germline assessment for Lynch syndrome. Extracted data included tumour testing, germline genetic testing, age, body mass index (BMI), family history, tumour stage, grade and histologic type. Associations between MMR-intact, MLH1 methylation positive, MMR-deficient and Lynch syndrome groups were analysed using descriptive statistics. The comprehensive search produced 4,400 publications, 29 met inclusion criteria. A total of 7,057 endometrial cancer cases were identified, 1,612 with abnormal immunohistochemistry, 977 with microsatellite instability. Nine-hundred patients underwent germline genetic testing, identifying 212 patients with Lynch syndrome. Patients in the Lynch syndrome and MMR-deficient groups were significantly younger than patients in the MMR-intact and MLH1 methylation positive groups. Patients with MMR-intact tumours had the highest BMI, followed by MMR-deficient, then Lynch syndrome. MMR-intact tumours were more likely to be grade I at diagnosis than other groups. Patients with Lynch syndrome and MMR-deficient tumours were less likely to have stage I disease as compared to patients with MMR-intact tumours. Endometrial cancer patients with MMR-deficient tumours have similar features to those with germline Lynch syndrome mutations, including age, grade, histology and stage. Even in the absence of a germline mutation, tumour evaluation for MMR status may have important clinical implications.
将DNA错配修复(MMR)评估纳入子宫内膜癌管理的护理标准,将导致错配修复缺陷且种系林奇综合征检测结果为阴性(MMR缺陷)的患者群体不断增加。在这项系统评价和研究中,对MMR完整、MLH1甲基化阳性、MMR缺陷或林奇综合征患者的子宫内膜癌临床病理特征进行了评估。对1990年至2018年期间在线数据库进行的系统检索,确定了对子宫内膜癌患者进行肿瘤检测(MMR蛋白免疫组织化学或微卫星不稳定性检测)以及林奇综合征种系评估的研究。提取的数据包括肿瘤检测、种系基因检测、年龄、体重指数(BMI)、家族史、肿瘤分期、分级和组织学类型。使用描述性统计分析MMR完整、MLH1甲基化阳性、MMR缺陷和林奇综合征组之间的关联。全面检索产生了4400篇出版物,29篇符合纳入标准。共确定了7057例子宫内膜癌病例,其中1612例免疫组织化学异常,977例微卫星不稳定性检测异常。900例患者进行了种系基因检测,确定了212例林奇综合征患者。林奇综合征组和MMR缺陷组患者明显比MMR完整组和MLH1甲基化阳性组患者年轻。MMR完整的肿瘤患者BMI最高,其次是MMR缺陷患者,然后是林奇综合征患者。MMR完整的肿瘤在诊断时更可能为I级,高于其他组。与MMR完整的肿瘤患者相比,林奇综合征和MMR缺陷的肿瘤患者患I期疾病的可能性较小。MMR缺陷的子宫内膜癌患者具有与种系林奇综合征突变患者相似的特征,包括年龄、分级、组织学和分期。即使在没有种系突变的情况下,对MMR状态进行肿瘤评估也可能具有重要的临床意义。