Summers Corinne, Sheth Vipul S, Bleakley Marie
Clinical Research Division, Fred Hutchinson Cancer Research Center, Seattle, WA, United States.
Department of Pediatrics, University of Washington, Seattle, WA, United States.
Front Pediatr. 2020 Jun 3;8:284. doi: 10.3389/fped.2020.00284. eCollection 2020.
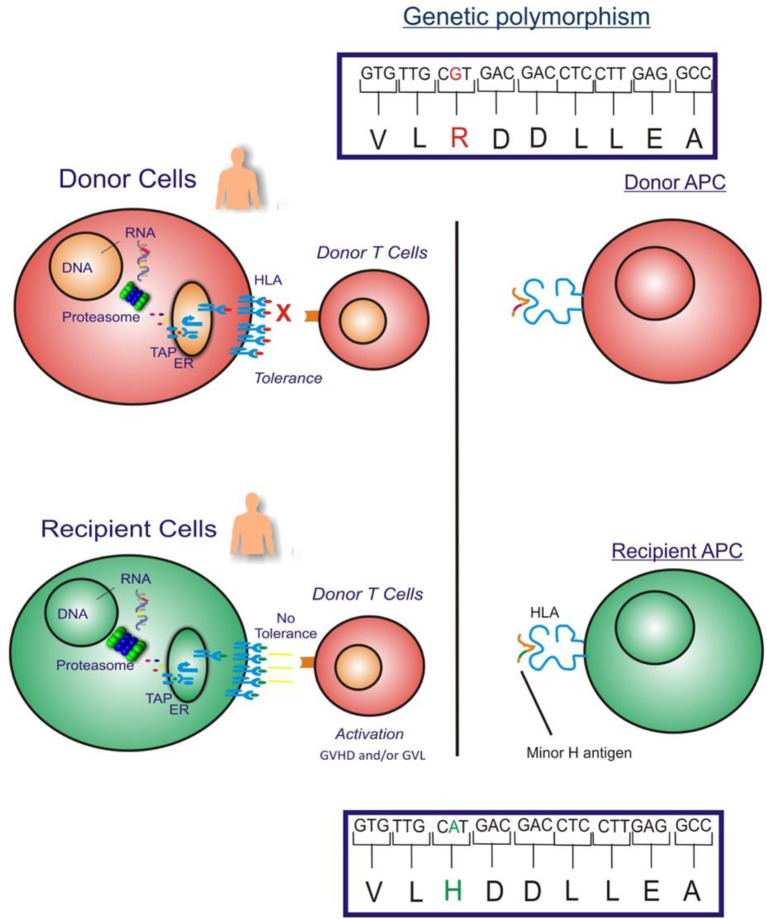
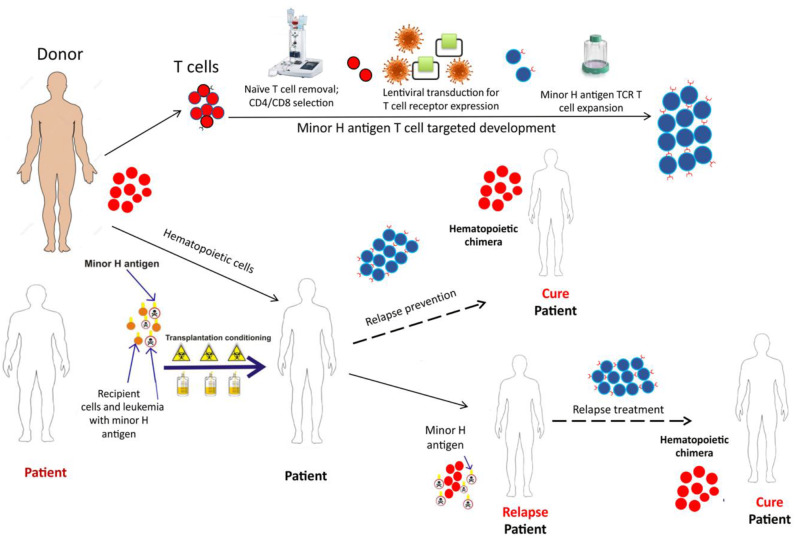
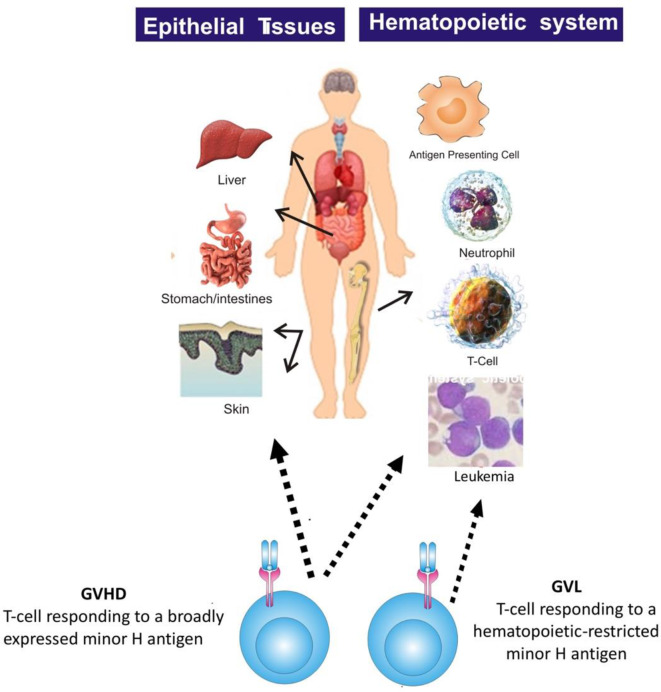
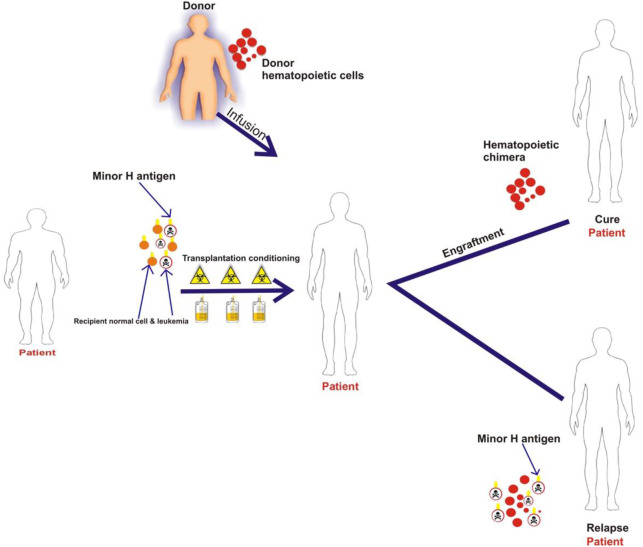
Minor Histocompatibility (H) antigens are major histocompatibility complex (MHC)/Human Leukocyte Antigen (HLA)-bound peptides that differ between allogeneic hematopoietic stem cell transplantation (HCT) recipients and their donors as a result of genetic polymorphisms. Some minor H antigens can be used as therapeutic T cell targets to augment the graft-vs.-leukemia (GVL) effect in order to prevent or manage leukemia relapse after HCT. Graft engineering and post-HCT immunotherapies are being developed to optimize delivery of T cells specific for selected minor H antigens. These strategies have the potential to reduce relapse risk and thereby permit implementation of HCT approaches that are associated with less toxicity and fewer late effects, which is particularly important in the growing and developing pediatric patient. Most minor H antigens are expressed ubiquitously, including on epithelial tissues, and can be recognized by donor T cells following HCT, leading to graft-vs.-host disease (GVHD) as well as GVL. However, those minor H antigens that are expressed predominantly on hematopoietic cells can be targeted for selective GVL. Once full donor hematopoietic chimerism is achieved after HCT, hematopoietic-restricted minor H antigens are present only on residual recipient malignant hematopoietic cells, and these minor H antigens serve as tumor-specific antigens for donor T cells. Minor H antigen-specific T cells that are delivered as part of the donor hematopoietic stem cell graft at the time of HCT contribute to relapse prevention. However, in some cases the minor H antigen-specific T cells delivered with the graft may be quantitatively insufficient or become functionally impaired over time, leading to leukemia relapse. Following HCT, adoptive T cell immunotherapy can be used to treat or prevent relapse by delivering large numbers of donor T cells targeting hematopoietic-restricted minor H antigens. In this review, we discuss minor H antigens as T cell targets for augmenting the GVL effect in engineered HCT grafts and for post-HCT immunotherapy. We will highlight the importance of these developments for pediatric HCT.
微小组织相容性(H)抗原是主要组织相容性复合体(MHC)/人类白细胞抗原(HLA)结合的肽段,由于基因多态性,同种异体造血干细胞移植(HCT)受者与其供者之间存在差异。一些微小H抗原可作为治疗性T细胞靶点,以增强移植物抗白血病(GVL)效应,从而预防或控制HCT后白血病复发。目前正在开发移植物工程和HCT后免疫疗法,以优化针对选定微小H抗原的T细胞递送。这些策略有可能降低复发风险,从而允许实施毒性较小、晚期效应较少的HCT方法,这在不断成长和发育的儿科患者中尤为重要。大多数微小H抗原在包括上皮组织在内的多种组织中普遍表达,HCT后可被供者T细胞识别,导致移植物抗宿主病(GVHD)以及GVL。然而,那些主要在造血细胞上表达的微小H抗原可作为选择性GVL的靶点。HCT后一旦实现完全供者造血嵌合,造血受限的微小H抗原仅存在于残留的受者恶性造血细胞上,这些微小H抗原作为供者T细胞的肿瘤特异性抗原。HCT时作为供者造血干细胞移植物一部分递送的微小H抗原特异性T细胞有助于预防复发。然而,在某些情况下,与移植物一起递送的微小H抗原特异性T细胞数量可能不足,或随着时间推移功能受损,导致白血病复发。HCT后,过继性T细胞免疫疗法可通过递送大量靶向造血受限微小H抗原的供者T细胞来治疗或预防复发。在本综述中,我们讨论了微小H抗原作为T细胞靶点在增强工程化HCT移植物中的GVL效应以及HCT后免疫治疗中的作用。我们将强调这些进展对儿科HCT的重要性。