Geriatric Psychiatrist, Minneapolis VA Health Care System, Mental Health Service Line, Minneapolis, MN, USA.
Assistant Professor, Department of Psychiatry, University of Minnesota, Minneapolis, MN, USA.
Transl Psychiatry. 2020 Jun 26;10(1):206. doi: 10.1038/s41398-020-00897-0.
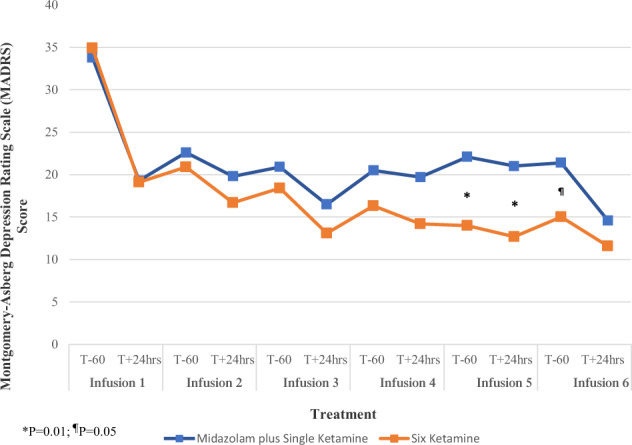
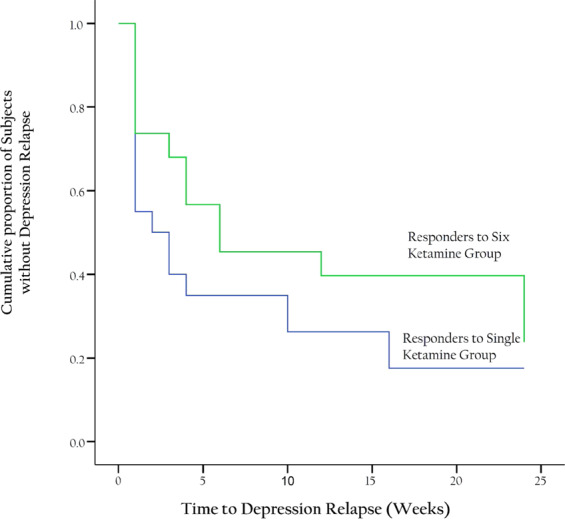
The strategy of repeated ketamine in open-label and saline-control studies of treatment-resistant depression suggested greater antidepressant response beyond a single ketamine. However, consensus guideline stated the lack of evidence to support frequent ketamine administration. We compared the efficacy and safety of single vs. six repeated ketamine using midazolam as active placebo. Subjects received either six ketamine or five midazolam followed by a single ketamine during 12 days followed by up to 6-month post-treatment period. The primary end point was the change from baseline in the Montgomery-Åsberg Depression Rating Scale (MADRS) score at 24 h after the last infusion. Fifty-four subjects completed all six infusions. For the primary outcome measure, there was no significant difference in change of MADRS scores between six ketamine group and single ketamine group at 24 h post-last infusion. Repeated ketamine showed greater antidepressant efficacy compared to midazolam after five infusions before receiving single ketamine infusion. Remission and response favored the six ketamine after infusion 4 and 5, respectively, compared to midazolam before receiving single ketamine infusion. For those who responded, the median time-to-relapse was nominally but not statistically different (2 and 6 weeks for the single and six ketamine group, respectively). Repeated infusions were relatively well-tolerated. Repeated ketamine showed greater antidepressant efficacy to midazolam after five infusions but fell short of significance when compared to add-on single ketamine to midazolam at the end of 2 weeks. Increasing knowledge on the mechanism of ketamine should drive future studies on the optimal balance of dosing ketamine for maximum antidepressant efficacy with minimum exposure.
在治疗抵抗性抑郁症的开放标签和生理盐水对照研究中,重复使用氯胺酮的策略表明,其抗抑郁反应优于单次氯胺酮。然而,共识指南指出,缺乏支持频繁使用氯胺酮的证据。我们比较了单次与六次重复氯胺酮使用咪达唑仑作为活性安慰剂的疗效和安全性。受试者接受六次氯胺酮或五次咪达唑仑治疗,随后在 12 天内接受单次氯胺酮治疗,随后进行长达 6 个月的治疗后随访。主要终点是末次输注后 24 小时内蒙哥马利-阿斯伯格抑郁评定量表(MADRS)评分的基线变化。54 名受试者完成了所有六次输注。对于主要结局指标,末次输注后 24 小时,六次氯胺酮组与单次氯胺酮组的 MADRS 评分变化无显著差异。与五次咪达唑仑相比,在接受单次氯胺酮输注前,重复氯胺酮显示出更大的抗抑郁疗效。与五次咪达唑仑相比,在接受单次氯胺酮输注前,四次和五次输注后重复氯胺酮的缓解率和反应率分别更优。对于那些有反应的患者,中位复发时间名义上但无统计学差异(单次和六次氯胺酮组分别为 2 周和 6 周)。重复输注相对耐受良好。与五次咪达唑仑相比,重复氯胺酮在五次输注后显示出更大的抗抑郁疗效,但与五次咪达唑仑后添加单次氯胺酮相比,在两周结束时未达到显著差异。增加对氯胺酮作用机制的了解,应推动未来关于最佳氯胺酮剂量平衡的研究,以实现最大的抗抑郁疗效和最小的暴露。