From the Department of Pharmacology, University of Virginia, Charlottesville (P.G.G., R.L.S., G.M.P.R.S., S.B.G.A.).
Department of Chemical Physiology and Biochemistry, Oregon Health & Sciences University, Portland (V.L.B.).
Hypertension. 2020 Aug;76(2):300-311. doi: 10.1161/HYPERTENSIONAHA.120.14521. Epub 2020 Jun 29.
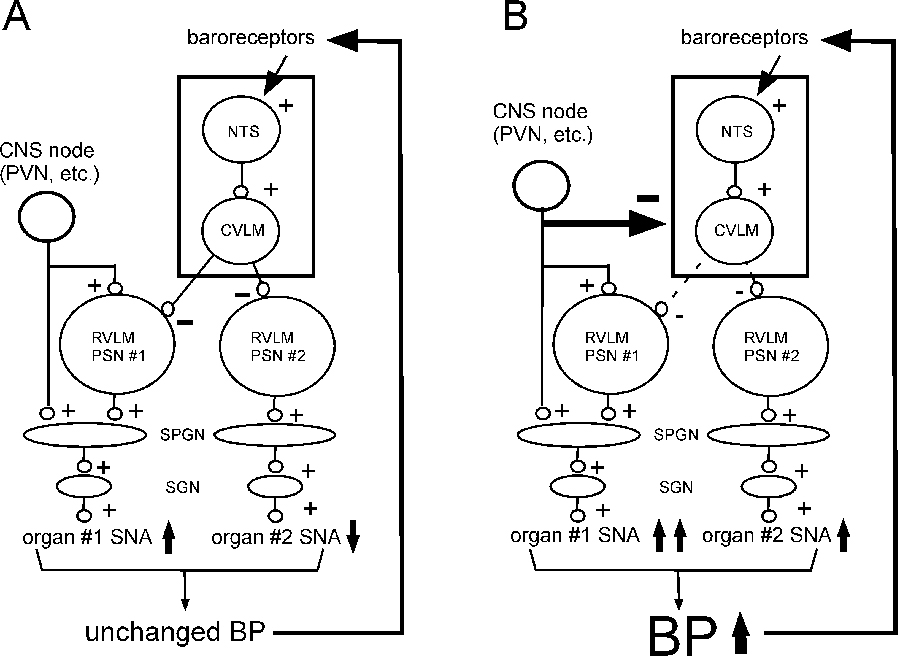
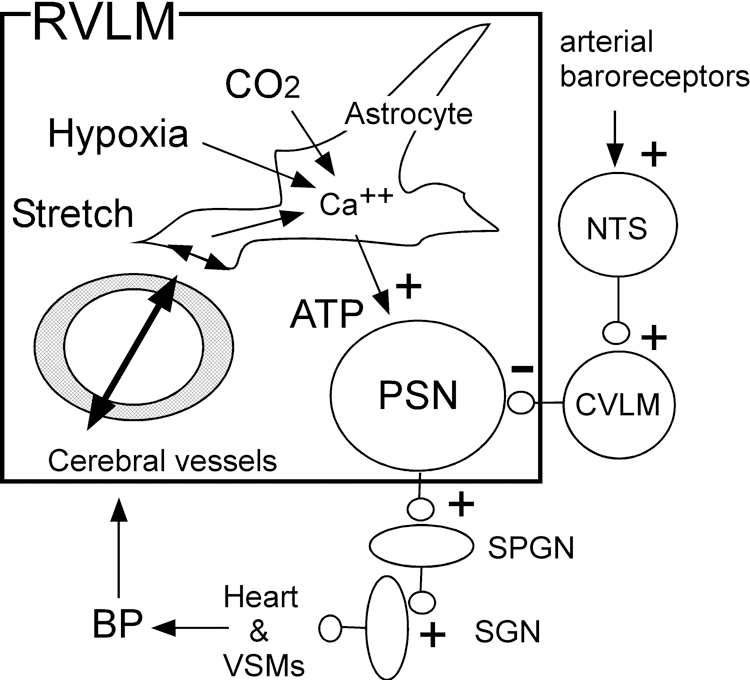
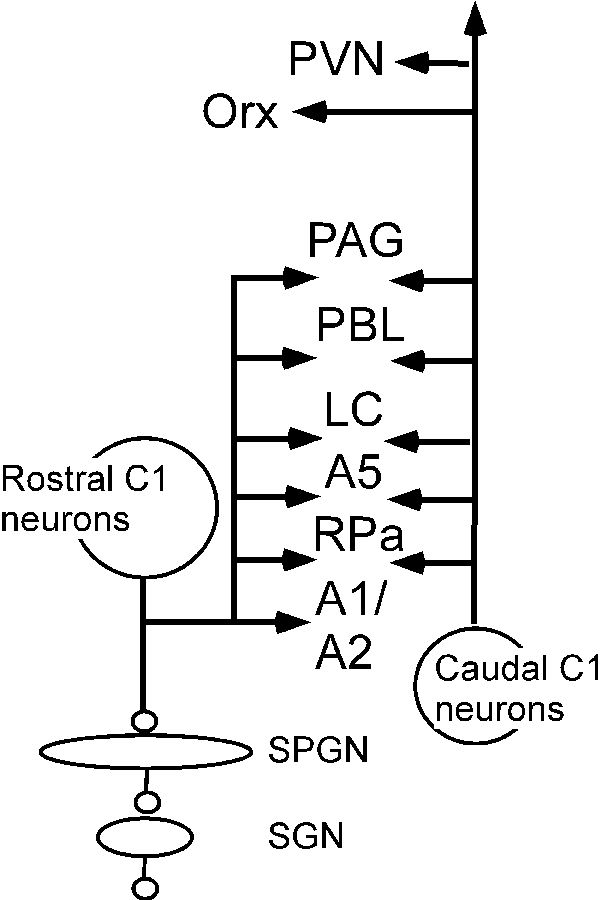
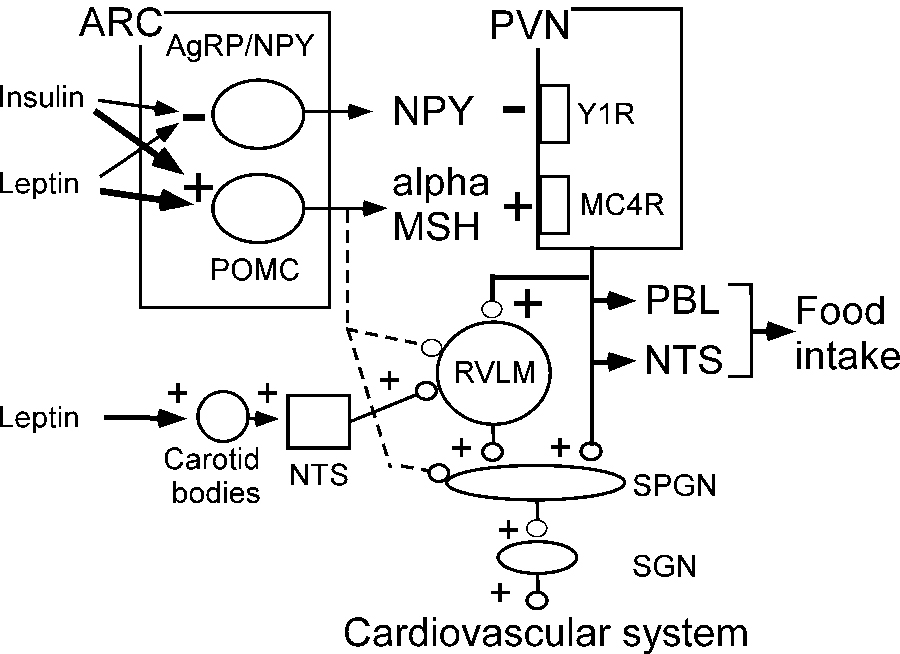
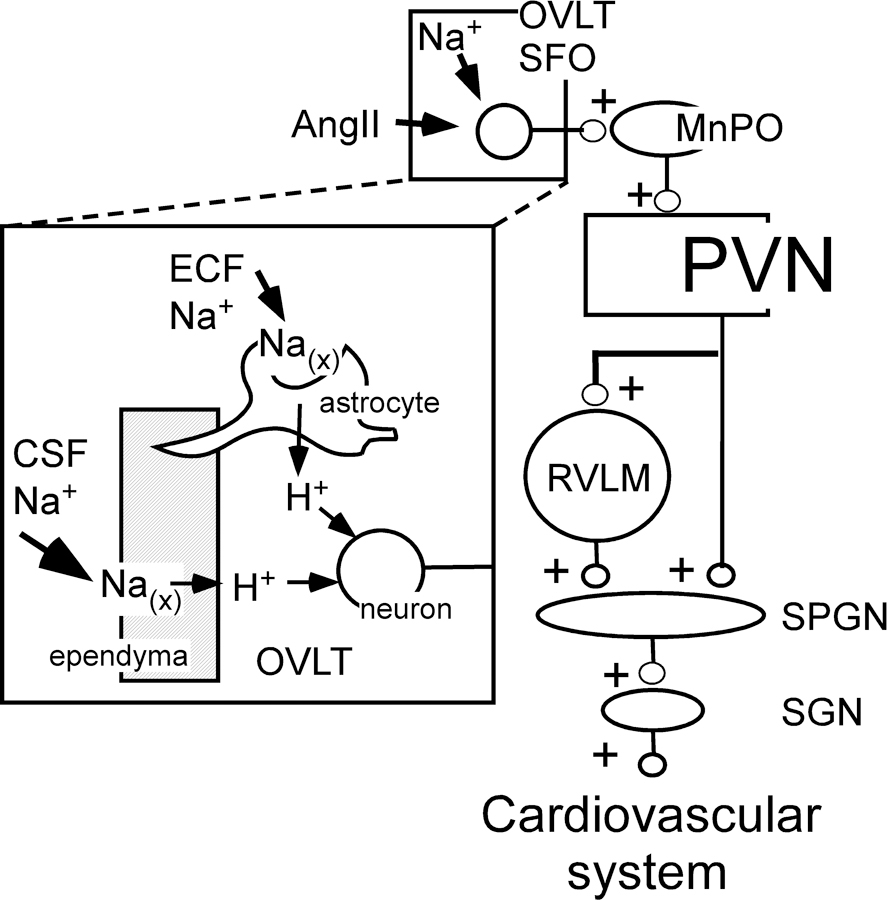
Neurogenic hypertension is associated with excessive sympathetic nerve activity to the kidneys and portions of the cardiovascular system. Here we examine the brain regions that cause heightened sympathetic nerve activity in animal models of neurogenic hypertension, and we discuss the triggers responsible for the changes in neuronal activity within these regions. We highlight the limitations of the evidence and, whenever possible, we briefly address the pertinence of the findings to human hypertension. The arterial baroreflex reduces arterial blood pressure variability and contributes to the arterial blood pressure set point. This set point can also be elevated by a newly described cerebral blood flow-dependent and astrocyte-mediated sympathetic reflex. Both reflexes converge on the presympathetic neurons of the rostral medulla oblongata, and both are plausible causes of neurogenic hypertension. Sensory afferent dysfunction (reduced baroreceptor activity, increased renal, or carotid body afferent) contributes to many forms of neurogenic hypertension. Neurogenic hypertension can also result from activation of brain nuclei or sensory afferents by excess circulating hormones (leptin, insulin, Ang II [angiotensin II]) or sodium. Leptin raises blood vessel sympathetic nerve activity by activating the carotid bodies and subsets of arcuate neurons. Ang II works in the lamina terminalis and probably throughout the brain stem and hypothalamus. Sodium is sensed primarily in the lamina terminalis. Regardless of its cause, the excess sympathetic nerve activity is mediated to some extent by activation of presympathetic neurons located in the rostral ventrolateral medulla or the paraventricular nucleus of the hypothalamus. Increased activity of the orexinergic neurons also contributes to hypertension in selected models.
神经原性高血压与肾脏和心血管系统部分区域的交感神经活动过度有关。在这里,我们研究了在神经原性高血压动物模型中引起交感神经活动增强的脑区,并讨论了导致这些区域神经元活动变化的触发因素。我们强调了证据的局限性,并在可能的情况下简要讨论了这些发现与人类高血压的相关性。动脉压力反射降低了动脉血压变异性,并有助于动脉血压设定点。通过新描述的血流依赖性和星形胶质细胞介导的交感神经反射,也可以升高这个设定点。这两个反射都集中在延髓头端的交感节前神经元上,都是神经原性高血压的可能原因。感觉传入功能障碍(减少压力感受器活动、增加肾或颈动脉体传入)导致多种形式的神经原性高血压。脑核或感觉传入的激活也可导致神经原性高血压,例如循环激素(瘦素、胰岛素、血管紧张素 II [血管紧张素 II])或钠过量。瘦素通过激活颈动脉体和弓状核的某些亚群来提高血管交感神经活性。血管紧张素 II 在终板内工作,可能在脑干和下丘脑的整个区域工作。钠主要在终板内被感知。无论其原因如何,过量的交感神经活动在一定程度上是通过位于延髓头端腹外侧或下丘脑室旁核的交感节前神经元的激活来介导的。在某些选定的模型中,食欲肽能神经元的活性增加也会导致高血压。