Morciano Marcello, Checkland Katherine, Billings Jenny, Coleman Anna, Stokes Jonathan, Tallack Charles, Sutton Matt
Health Organisation, Policy and Economics (HOPE) Research Group, University of Manchester, Manchester, M13 9PL, United Kingdom.
Health Organisation, Policy and Economics (HOPE) Research Group, University of Manchester, Manchester, M13 9PL, United Kingdom.
Health Policy. 2020 Aug;124(8):826-833. doi: 10.1016/j.healthpol.2020.06.004. Epub 2020 Jun 10.
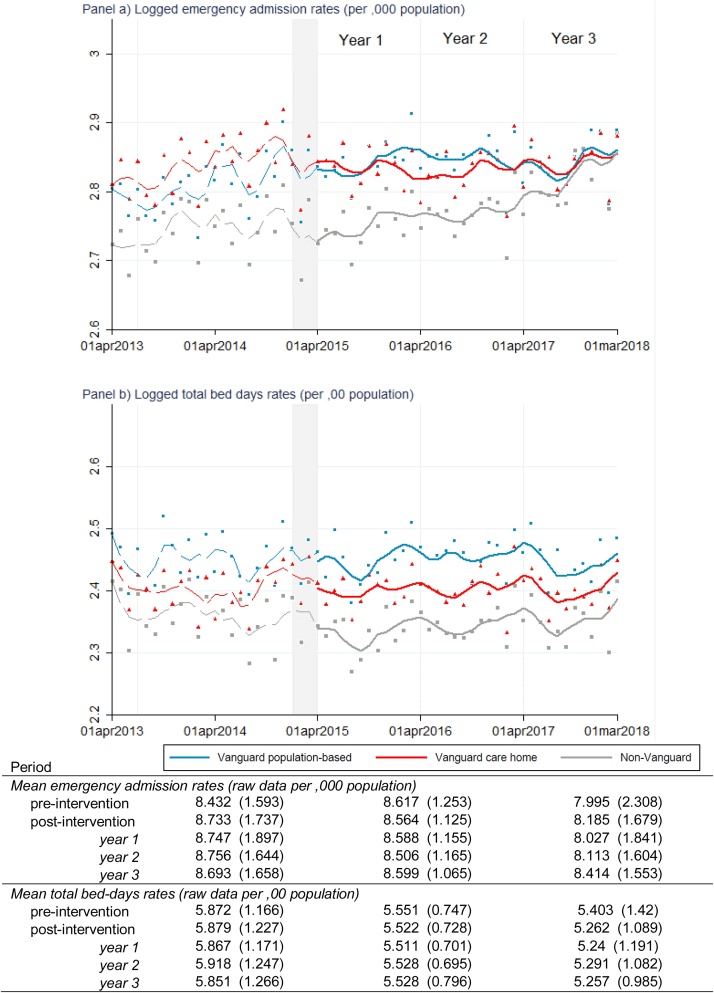
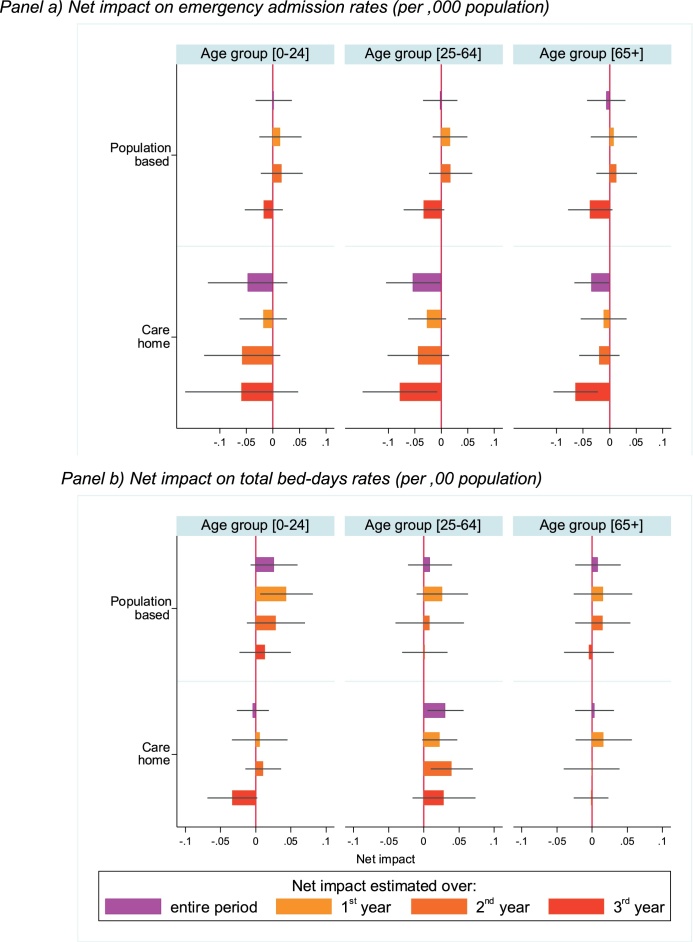
Closer integration of health and social care services has become a cornerstone policy in many developed countries, but there is still debate over what population and service level is best to target. In England, the 2019 Long Term Plan for the National Health Service included a commitment to spread the integration prototypes piloted under the Vanguard `New Care Models' programme. The programme, running from 2015 to 2018, was one of the largest pilots in English history, covering around 9 % of the population. It was largely intended to design prototypes aimed at reducing hospital utilisation by moving specialist care out of hospital into the community and by fostering coordination of health, care and rehabilitation services for (i) the whole population ('population-based sites'), or (ii) care home residents ('care home sites'). We evaluate and compare the efficacy of the population-based and care home site integrated care models in reducing hospital utilisation. We use area-level monthly counts of emergency admissions and bed-days obtained from administrative data using a quasi-experimental difference-in-differences design. We found that Vanguard sites had higher hospital utilisation than non-participants in the pre-intervention period. In the post-intervention period, there is clear evidence of a substantial increase in emergency admissions among non-Vanguard sites. The Vanguard integrated care programme slowed the rise in emergency admissions, especially in care home sites and in the third and final year. There was no significant reduction in bed-days. In conclusion, integrated care policies should not be relied upon to make large reductions in hospital activity in the short-run, especially for population-based models.
卫生与社会护理服务的更紧密整合已成为许多发达国家的一项核心政策,但对于最佳的目标人群和服务水平仍存在争议。在英国,2019年国民健康服务长期计划承诺推广在“先锋‘新护理模式’”项目下试点的整合模式。该项目于2015年至2018年实施,是英国历史上规模最大的试点项目之一,覆盖了约9%的人口。其主要目的是设计一些模式,旨在通过将专科护理从医院转移到社区,并促进针对(i)全体人口(“基于人群的场所”)或(ii)养老院居民(“养老院场所”)的健康、护理和康复服务的协调,来降低医院利用率。我们评估并比较了基于人群的场所和养老院场所的整合护理模式在降低医院利用率方面的效果。我们使用准实验性差异中的差异设计,从行政数据中获取地区层面每月的急诊入院人数和住院天数计数。我们发现,在干预前期,先锋场所的医院利用率高于非参与者。在干预后期,有明确证据表明非先锋场所的急诊入院人数大幅增加。先锋整合护理项目减缓了急诊入院人数的上升,尤其是在养老院场所和第三年及最后一年。住院天数没有显著减少。总之,短期内不应依赖整合护理政策来大幅减少医院业务量,特别是对于基于人群的模式。