Department of Medicine, Division of Nephrology, University Health Network, Toronto, Ontario, Canada.
Department of Medicine, Division of Medical Oncology and Hematology, University Health Network, Toronto, Ontario, Canada.
J Immunother Cancer. 2020 Jun;8(1). doi: 10.1136/jitc-2019-000467.
Immune checkpoint inhibitors (ICPi) are a novel and promising anti-cancer therapy. There are limited data on the incidence, risk factors and outcomes of acute kidney injury (AKI) in patients receiving ICPi.
We conducted a cohort study of patients receiving ICPi at our center between 2010 and 2017 via electronic health record. The primary outcome was AKI (increase of >50% from baseline serum creatinine (sCr)). Risk factors for AKI were assessed using logistic regression. Survival among those with and without AKI was compared using the Kaplan-Meier method.
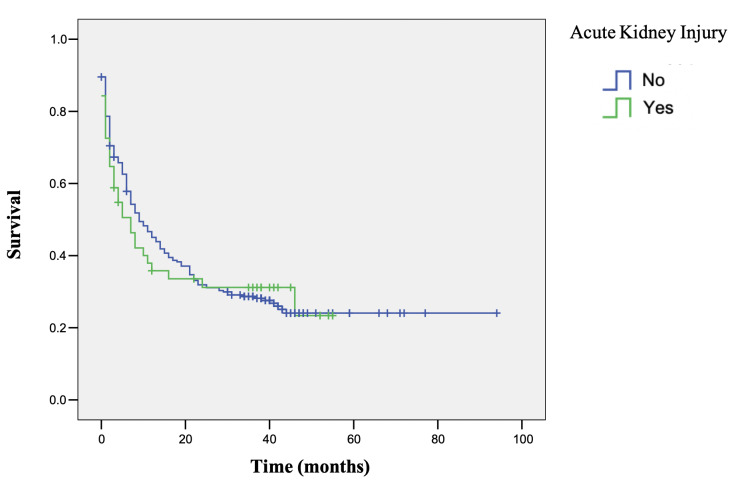
Among 309 patients on ICPi, 51 (16.5%) developed AKI (Kidney Disease Improving Global Outcomes (KDIGO) stages 1: 53%, 2: 22%, 3: 25%). AKI was associated with other immune-related adverse events (IRAE) (OR 3.2, 95% CI 1.6 to 6; p<0.001), hypertension (OR 4.3, 95% CI 1.8 to 6.1; p<0.001) and cerebrovascular disease (OR 9.2; 95% CI 2.1 to 40; p<0.001). Baseline sCr, cancer, and ICPi type was not associated with AKI. Use of angiotensin-converting enzyme inhibitors/angiotensin-receptor blockers (OR 2.9; 95% CI 1.5 to 5.7; p=0.002), diuretics (OR 4.3; 95% CI 1.9 to 9.8; p<0.001), and corticosteroid treatment (OR 1.9; 95% CI 1.1 to 3.6; p=0.03) were associated with AKI. In the multivariable analysis, AKI was associated only with other IRAE (OR 2.82; 95% CI 1.45 to 5.48; p=0.002) and hypertension (OR 2.96; 95% CI 1.33 to 6.59; p=0.008). AKI was not associated with increased risk of mortality (HR 1.1; 95% CI: 0.8 to 1.6; p=0.67). ICPi nephrotoxicity was attributed via biopsy or nephrologist assessment in 12 patients (six interstitial nephritis, two membranous nephropathy, two minimal change disease, and two thrombotic microangiopathy). Subsequent doses of ICPi were administered to 12 patients with prior AKI, with one (8.3%) having recurrent AKI.
AKI is a common complication in patients receiving ICPi treatment. The development of other IRAE and previous diagnosis of hypertension were associated with increased AKI risk. AKI was not associated with worse survival. Distinguishing kidney IRAE from other causes of AKI will present a frequent challenge to oncology and nephrology practitioners. Kidney biopsy should be considered to characterize kidney lesions and guide potential therapy.
免疫检查点抑制剂(ICPi)是一种新型且有前途的抗癌疗法。关于接受 ICPi 治疗的患者发生急性肾损伤(AKI)的发生率、风险因素和结局,数据有限。
我们通过电子病历对 2010 年至 2017 年期间在我们中心接受 ICPi 治疗的患者进行了队列研究。主要结局为 AKI(血清肌酐(sCr)基线增加>50%)。使用逻辑回归评估 AKI 的风险因素。使用 Kaplan-Meier 方法比较有和无 AKI 患者的生存率。
在 309 名接受 ICPi 治疗的患者中,51 名(16.5%)发生 AKI(肾脏病改善全球结局(KDIGO)分期 1:53%,2:22%,3:25%)。AKI 与其他免疫相关不良事件(IRAE)相关(OR 3.2,95%CI 1.6 至 6;p<0.001)、高血压(OR 4.3,95%CI 1.8 至 6.1;p<0.001)和脑血管疾病(OR 9.2;95%CI 2.1 至 40;p<0.001)。基线 sCr、癌症和 ICPi 类型与 AKI 无关。血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂的使用(OR 2.9;95%CI 1.5 至 5.7;p=0.002)、利尿剂(OR 4.3;95%CI 1.9 至 9.8;p<0.001)和皮质类固醇治疗(OR 1.9;95%CI 1.1 至 3.6;p=0.03)与 AKI 相关。在多变量分析中,AKI 仅与其他 IRAE(OR 2.82;95%CI 1.45 至 5.48;p=0.002)和高血压(OR 2.96;95%CI 1.33 至 6.59;p=0.008)相关。AKI 与死亡率增加无关(HR 1.1;95%CI:0.8 至 1.6;p=0.67)。通过活检或肾病医生评估,将 12 名患者(6 名间质性肾炎、2 名膜性肾病、2 名微小病变性肾病和 2 名血栓性微血管病)的 ICPi 肾毒性归因于 ICPi。在先前有 AKI 的 12 名患者中继续给予 ICPi 治疗,其中 1 名(8.3%)再次发生 AKI。
AKI 是接受 ICPi 治疗的患者的常见并发症。其他 IRAE 的发生和高血压的既往诊断与 AKI 风险增加相关。AKI 与生存结局较差无关。区分肾 IRAE 与其他 AKI 原因将对肿瘤学和肾脏病学医生提出频繁的挑战。应考虑进行肾脏活检以确定肾脏病变并指导潜在的治疗。